
COVID-19 / Malicious Medical Quackery
[Ed.: FEAR YOUR DOCTOR! Medicine is a disgraced profession. They cannot (and must not) be trusted any longer!
Cultivate Nosocomephobia and iatrophobia. Spread ‘vaccine hesitancy’! How Bad is My Batch? Enter your batch number(s) and find out. Then take action and purge yourself of this shit to the extent possible. It’s do-able!
If you know someone injured by the jabs, direct them to humanitysuit.com to become a plaintiff. Another great legal resource is: Freedom Council https://freedomcounsel.org; For Vaccine Exemptions: https://www.sirillp.com/vaccine-exemption-attorneys/ .
RESOURCE: VACCINE INFO COURSE All material from the course has been transferred to telegram. You can access everything here]
DIED SUDDENLY: Official Documentary Film [1:17:21]
Inside mRNA Vaccines – The Movie [1:00:59]
Premiered Aug 11, 2025
This film explores the unprecedented global rollout of mRNA vaccine technology. www.insidemrnavaccines.com
00:00 Intro
02:53 Surgeon Joel Wallskog’s health issues
06:21 Operation Warp Speed initiative
06:38 Former CDC Director on mRNA vaccines
07:35 Regulators’ safety assessment
08:09 Calls to pause mRNA vaccines
09:32 mRNA researcher Robert Malone
12:56 Pathologist Ryan Cole on COVID vaccination
14:14 Cardiologist Aseem Malhotra on heart health
14:37 Cardiologist Peter McCullough on side effects
17:28 Scientist Jessica Rose on vaccine concerns
18:41 Critical care specialist Paul Marik on patient community
21:17 Explaining mRNA
23:45 How mRNA vaccines work
27:06 Spike protein and possible effects
30:57 Pathologist Arne Burkhardt’s biopsy findings
32:49 Health agencies’ safety stance
33:38 Vaccination in pregnancy and children
34:22 Artist Jessica Sutta’s health issues
39:03 Future uses of mRNA technology
42:55 Tobie Vergara’s health issues
45:12 History of mRNA vaccines
46:44 Modified mRNA technology
48:40 mRNA research status in 2017
49:07 Toxicity concerns in 2017
49:33 Progress in mRNA technology
49:50 mRNA vaccines during the pandemic
55:41 Support for post-vaccination syndrome
57:06 Doctors offering assistance
[Ed.: Other vaccine controversies include:
1. How the vaccines caused the paralysis of polio
2. How vaccines caused sudden infant death syndrome (SIDS)
3. How vaccines cause brain damage, but we call it autism
4. How we covered up brain damage and made it a mental condition
Bombshell Vax vs. Unvax Study Finally Sees the Light of Day — And the Results Are Staggering
[Ed.: An Inconvenient Study Full Movie [1:20:36]
Here is the link to the documentary An Inconvenient Study, which premiered tonight at the Malibu Film Festival. It is the brilliant true story of the suppression of a vaxed vs unvaxed children’s study and the Henry Ford Health Center–suppressed because it showed over several years 3-6 TIMES the incidence of chronic illness between children who had even ONE childhood vaccine compared with children compared with children who had NO vaccines. PLUS there was ZERO autism, ADHD and a couple of other things in the unvaxed cohort.
Watch the entire video and be sure to share it with everyone you think SHOULD KNOW about what it shows!
New Studies Link mRNA “Vaccines” to Severe Neurological Damage, Genomic Integration, and Turbo Cancer — While HHS Remains Silent [VIDEO 19:20] NICOLAS HULSCHER, MPH
Epidemiologist Nicolas Hulscher joins Breanna Morello on InfoWars
NOV 07, 2025
Today, I joined Breanna Morello on InfoWars to discuss our new peer-reviewed study that found catastrophic neurological injury from the COVID-19 mRNA injections.
63 serious safety signals were identified — all involving the central nervous system — including encephalitis, meningitis, myelitis, demyelination syndromes, brain/spinal cord abscesses, and even Creutzfeldt–Jakob (prion) disease, which appeared 847× more likely after COVID-19 mRNA shots than after traditional vaccines.
The Dark Truth About Vaccines – Del Bigtree Exposes the Unthinkable [7:39] LIONESS OF JUDAH MINISTRY
“This isn’t science—it’s a witch cult.”
November 7, 2025
Source: RogerHodkinson
Del Bigtree: “We’re injecting our kids with aborted fetal DNA, chopped-up organs from 3-month-old babies—76 in one study—admitted by vaccine chief Stanley Plotkin himself.
Monkey kidneys, hamster cells, cancer lines, mercury, formaldehyde… it’s a cauldron of horrors even Shakespeare couldn’t imagine.
And the worst part?
They admit: ‘We never studied this. We don’t know what it does.’
This isn’t science—it’s a witch cult.”
Dr. Stanley Plotkin – Vaccine Ingredients
Dr. Stanley Plotkin, widely recognized as a leading authority in vaccinology, discusses some of the “healthy” ingredients in vaccines.
How many pediatricians know this?
If they know this, how can they believe this is healthy?
WATCH [7:39]
Can leucovorin cure autism? Meet the moms determined to find out MATT HIMES
When it comes to medical breakthroughs, parental love has an impressive track record.
NOVEMBER 07, 2025 Blaze Media
A humble, decades-old folate compound — used not to fight cancer but to ease the side effects of chemotherapy — has become the latest flashpoint in America’s health wars.
On September 10, the Trump administration announced that the FDA would move toward approving leucovorin for children with cerebral folate deficiency, a rare metabolic disorder linked to autism in some cases. Supporters hailed it as long-overdue recognition of promising small studies; critics called it another example of the MAHA agenda politicizing science.
While bureaucrats and scientists bicker, families with real skin in the game tirelessly run their own experiments and share their results, hoping the science will eventually catch up.
The debate since has been fierce, with professional groups such as the American Academy of Pediatrics advising against the off-label use of leucovorin for autism, warning that the evidence remains preliminary — while prominent physicians call for larger, biomarker-guided trials to confirm what early studies suggest.
A parent’s love
All parties insist their motives are pure, but this latest skirmish is a reminder of how tangled those motives can be. What drives the people and institutions pushing medical science forward is often a sincere desire to help people, yes — mixed in with ambition, rivalry, financial interest, and the unspoken urge to be the one who’s right.
But there’s another force at work here, deeper and simpler, and it tends to override all the rest: a parent’s love for a child.
This is the same love that kept the parents of children with cystic fibrosis pushing to understand a condition doctors considered hopeless, or that led a Hollywood father to resurrect a forgotten epilepsy therapy to help his son. And now it’s the force animating hundreds of parents who believe a decades-old folate compound has literally given their autistic children a voice.
While bureaucrats and scientists bicker, families with real skin in the game tirelessly run their own experiments and share their results, hoping the science will eventually catch up.
Even before the FDA signaled approval of leucovorin for cerebral folate deficiency — a rare metabolic disorder with links to autism — parents have been sharing reports of progress with the drug on Reddit forums and in Facebook groups to share anecdotal reports of progress. A few families have also told their stories in clinic-produced or news-segment videos.
A treatment’s hope
Leucovorin, also called folinic acid, is a bioactive form of folate. It’s been used for decades to “rescue” patients from high-dose chemotherapy. In autism, it’s being repurposed to bypass what some researchers call a “folate transport blockade.”
Up to 70% of autistic children in certain studies test positive for folate receptor alpha autoantibodies — immune proteins that prevent folate from reaching the brain. The result: cerebral folate deficiency. High-dose folinic acid appears to restore that supply, sometimes with striking behavioral effects.
Dr. Richard Frye, a pediatric neurologist at Phoenix Children’s Hospital, led one of the first controlled trials in 2016. His team found improved verbal communication in FRAA-positive children treated with leucovorin. Later case studies described language bursts, better eye contact, and calmer affect.
From ‘no words’ to the Pledge of Allegiance
The parents themselves provide more affecting testimony. Carolyn Connor’s son Mason was 1 when she realized something was amiss: “He wasn’t talking. No language. No words.”
When their pediatrician downplayed this lag in development as typical in boys, she and her husband began doing their own research, which led them to Frye. Three days after starting leucovorin, Mason spoke his first words.
Now 6, he continues to take the medication, and continues to thrive.
Beth Ann Kersse’s daughter was diagnosed with autism at age 3. “In her vocabulary she had about three or four words,” Kersse said in a video uploaded by Washington, D.C.-based Potomac Psychiatry.
“But she didn’t call me ‘Mom.’ She kind of would point at me,” she added.
That’s when Kersse and her husband began exploring leucovorin. Two years later, Kersse describes her almost 5-year-old daughter’s transformation as “incredible.”
“The other day she stood up and put her hand over her heart, and she recited the Pledge of Allegiance, and we were just like, OK … I didn’t know we knew that. … She’s able to have a full conversation; she can tell us how she’s feeling.”
Late last month, Nebraska pediatrician Dr. Phil Boucher posted a case study detailing how a 3.5-year-old autistic girl responded to leucovin treatment, citing texts from her mother reporting that she was “blown away” by the changes she observed:
She is starting to consistently look at people when they call her name. … She’s becoming more interested in her little sister. … She also has started taking some of the baby dolls that we have and has been covering them up with a blanket, giving them a kiss, and saying, “Night night.”
As Boucher is careful to point out, anecdotal success stories like these don’t prove the drug works. But to those experiencing the improvement firsthand, they’re a promising sign that a simple, inexpensive vitamin derivative can do what years of therapy can’t.
And if this promise does indeed bear fruit, leucovorin treatment will be the latest of many homegrown revolutions in medical care spearheaded by determined mothers and fathers unwilling to wait for consensus.
RELATED CONTENT
It’s the testosterone, stupid!
The poisoned stream of culture is flowing through our churches
Global chip dispute threatens auto production again!
Tylenol fights autism claims, slams proposed FDA warning label as ‘unsupported’ by science
MATT HIMES Matt Himes is the managing editor for Align.
Breaking down the facts behind the headlines — and why the real risk lies in scientific illiteracy, not melatonin.
NOV 06, 2025
Read, share, and comment on the X post dedicated to this article here: https://x.com/sayerjigmi/status/1986629181216821364
Last week, the American Heart Association (AHA) issued a press release titled, “Long-term use of melatonin supplements to support sleep may have negative health effects.” The headline alone was enough to ripple across health media, stirring anxiety among millions who rely on melatonin for sleep support.
But beneath the alarmist phrasing lies a truth far more mundane—and more troubling. The study behind the headline isn’t a peer-reviewed paper at all. It’s a conference abstract, a short presentation of unverified data shared at the AHA’s annual meeting. In other words: a preview, not proof.
The Anatomy of a Press Release Panic
The AHA release describes an analysis of over 130,000 patients with chronic insomnia whose electronic health records (EHRs) were examined through the TriNetX Global Research Network. Researchers claimed that those taking melatonin for at least a year were:
- 90% more likely to be diagnosed with heart failure
- 3.5× more likely to be hospitalized for it
- Nearly twice as likely to die from any cause
Numbers like that would make melatonin sound more dangerous than cigarettes. And yet, the AHA’s own fine print quietly states:
“This study cannot prove a direct cause-and-effect relationship.”
“The findings are considered preliminary until published in a peer-reviewed journal.”
That should have been the headline.
The Media Echo Chamber of Fear & Distortion
Within hours, the world’s major news outlets reproduced the AHA’s talking points almost verbatim. The New York Times, CNN, USA Today, Healthline, People, and Fox News all issued headlines warning that “long-term melatonin use is linked to heart problems” or that melatonin users face a “90% higher risk of heart failure.”
These headlines are textbook hyperbole—amplifying a non-causal, non-peer-reviewed finding into a sweeping medical warning. None of these outlets explained that the data were drawn from incomplete EHR records, that “melatonin use” referred only to prescription cases (not the far larger over-the-counter population), or that the researchers explicitly stated their results cannot establish causality.
This is how science by press release becomes science by soundbite. The public never reads the caveats; they only see the fear.
A Study Designed to Confuse
When we dig into the methods, the implausibility becomes obvious.
The study only counted people with a prescription for melatonin—which is common in the U.K. but almost nonexistent in the U.S., where melatonin is sold over the counter. As the authors admit:
“Everyone taking it as an over-the-counter supplement… would have been in the non-melatonin group.”
This means that millions of people who actually use melatonin nightly were classified as non-users, while the so-called “melatonin group” was composed almost entirely of patients sick enough to have their sleep problems documented and treated in medical systems requiring prescriptions.
That’s not a safety signal — it’s a statistical illusion.
Confounding, Not Causation
Even if the data were reliable, the confounders are overwhelming. Chronic insomnia often travels with anxiety, depression, hypertension, and metabolic dysfunction — each a major risk factor for cardiovascular disease. Matching patients by demographics or comorbidities doesn’t erase the underlying severity bias: those who seek prescriptions tend to be those who are already unwell.
Moreover, the researchers lacked basic data on:
- Sleep quality and circadian rhythm disruption
- Lifestyle factors (diet, alcohol, shift work, screen exposure)
- Supplement dosage and purity
- Psychiatric medications used concurrently
Without these, there’s no meaningful inference about melatonin itself.
Moreover, the study failed to account for several key pharmacological confounders. While the authors excluded patients taking benzodiazepines, they did not control for other pharmaceutical sleep drugs such as zolpidem (Ambien), eszopiclone (Lunesta), or trazodone — all of which carry well-documented cardiometabolic risks. Nor did they adjust for the use of statins, SSRIs, or antihypertensives, which are both common among insomnia patients and known to alter cardiovascular function (learn more about the cardiotoxicity of statin drugs) and sleep architecture. Failing to isolate these variables makes it virtually impossible to determine whether the observed risks stem from melatonin itself or from concurrent drug exposure.
The Biological Reality: Melatonin as a Protector
For decades, melatonin has been one of the most studied molecules in the realm of oxidative stress and cardiometabolic protection. Peer-reviewed studies have shown that it:
- Reduces blood pressure and improves endothelial function
- Protects mitochondria and heart tissue after ischemic injury
- Mitigates oxidative damage and inflammation across numerous organs
A 2022 meta-analysis in the Journal of Pineal Research found melatonin to be broadly cardioprotective, not cardiotoxic.
This aligns with the GreenMedInfo research database, which has indexed nearly 1,000 studies on melatonin’s diverse physiological benefits across more than 400 health conditions, and documents up to 130 distinct pharmacological actions of the molecule — including antioxidant, anti-inflammatory, neuroprotective, and cardioprotective effects (see the research compendium here).
NOV 06, 2025
In this post I am republishing a blog post from HackerNoon, June 24, 2025 by Tim Hinchliffe, Editor, The Sociable. It is very well researched and sourced material showing that the Pentagon (DARPA) is funding AI-modeling programs in order to fake future pandemics with greater ease.
DARPA is getting into the business of simulating disease outbreaks, including modeling interventions such as mass vaccination campaigns, lockdowns, and communication strategies.
Last week [mid-June, 2025], the US Defense Advanced Research Projects Agency (DARPA) put out a Request for Information (RFI) seeking information regarding “state-of-the-art capabilities in the simulation of disease outbreaks.”
The Pentagon’s research and development funding arm wants to hear from academic, industry, commercial, and startup communities on how to develop “advanced capabilities that drive technical innovation and identify critical gaps in bio-surveillance, diagnostics, and medical countermeasures” in order to “improve preparedness for future public health emergencies.”
“Intervention Strategies: Detail the range of intervention strategies that can be modeled, including (but not limited to) vaccination campaigns, social distancing measures, quarantine protocols, treatments, and public health communication strategies. Specifically, describe the ability to model early intervention and its impact on outbreak trajectory”
DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025
As if masks, social distancing, lockdowns, and vaccination mandates under the unscientific guise of slowing the spread and preventing the transmission of COVID weren’t harmful enough, the US military wants to model the effects of these exact same countermeasures for future outbreaks.
The RFI also asks participants “Fatality Rate & Immune Status: How are fatality rates and varying levels of population immunity (natural or vaccine-induced) incorporated into your simulations?“
Does “natural or vaccine-induced” relate to “population immunity” or “fatality rates” or both?
Moving on, the RFI gets into modeling lockdowns, social distancing, and mass vaccination campaigns, along with communication strategies:
“Intervention Strategies: Detail the range of intervention strategies that can be modeled, including (but not limited to) vaccination campaigns, social distancing measures, quarantine protocols, treatments, and public health communication strategies. Specifically, describe the ability to model early intervention and its impact on outbreak trajectory.“
The fact that DARPA wants to model these so-called intervention strategies just after the entire world experienced them suggests that these exact same measures will most likely be used again in the future.
“We are committed to developing advanced modeling capabilities to optimize response strategies and inform the next generation of (bio)technology innovations to protect the population from biological threats. We are particularly focused on understanding the complex interplay of factors that drive outbreak spread and evaluating the effectiveness of potential interventions.”
DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025
“Identification of optimal timelines and capabilities to detect, identify, attribute, and respond to disease outbreaks, including but not limited to biosensor density deployment achieving optimal detection timelines, are of interest”
DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025
With lockdowns, mass vaccination campaigns, and social distancing still on the table from the last around, it appears that AI and Machine Learning will play a much bigger role in the next.
For future innovation, the DARPA RFI asks applicants to: “Please describe any novel technical approaches – or applications of diverse technical fields (e.g., machine learning, artificial intelligence, complex systems theory, behavioral science) – that you believe would significantly enhance the state-of-the-art capabilities in this field or simulation of biological systems wholistically.”
Instead of putting a Dr. Fauci, a Dr. Birx, a replaceable CDC director, a TV doctor, a big pharma CEO, or a Cuomo brother out there to lie to your face about how they were all just following The ScienceTM, why not use AI and ML and combine them with behavioral sciences in order to concoct your “public health communications strategies?”
When you look at recently announced DARPA programs like Kallisti and MAGICS, which are aimed at creating an algorithmic Theory of Mind to model, predict, and influence collective human behavior, you start to get a sense of how all these programs can interweave.
“The MAGICS ARC calls for paradigm-shifting approaches for modeling complex, dynamic systems for predicting collective human behavior”
DARPA, MAGICS ARC, April 2025
On April 8, DARPA issued an Advanced Research Concepts (ARC) opportunity for a new program called “Methodological Advancements for Generalizable Insights into Complex Systems (MAGICS)” that seeks “new methods and paradigms for modeling collective human behavior.”
Nowhere in the MAGICS description does it mention modeling or predicting the behavior of “adversaries” as is DARPA’s custom.
Instead, it talks at length about “modeling human systems,” along with anticipating, predicting, understanding, and forecasting “collective human behavior” and “complex social phenomena” derived from “sociotechnical data sets.”
Could DARPA’s MAGICS program be applied to simulating collective human behavior when it comes to the next public health emergency, be it real or perceived?
“The goal of an upcoming program will be to develop an algorithmic theory of mind to model adversaries’ situational awareness and predict future behavior”
DARPA, “Theory of Mind” Special Notice, December 2024
In December 2024, DARPA launched a similar program called Theory of Mind, which was renamed Kallisti a month later.
The goal of Theory of Mind is to develop “new capabilities to enable national security decisionmakers to optimize strategies for deterring or incentivizing actions by adversaries,” according to a very brief special announcement.
DARPA never mentions who those “adversaries” are. In the case of a public health emergency, an adversary could be anyone who questions authoritative messaging.
The Theory of Mind program will also “seek to combine algorithms with human expertise to explore, in a modeling and simulation environment, potential courses of action in national security scenarios with far greater breadth and efficiency than is currently possible.
“This would provide decisionmakers with more options for incentive frameworks while preventing unwanted escalation.”
“We are interested in a comprehensive overview of current and emerging technologies for disease outbreak simulation, how simulation approaches could be extended beyond standard modeling methods, and to understand how diseases spread within and between individuals including population level dynamics”
DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025
They say that all the modeling and simulating across programs is for “national security,” but that is a very broad term.
DARPA is in the business of R&D for national security purposes, so why is the Pentagon modeling disease outbreaks and intervention strategies while simultaneously looking to predict and manipulate collective human behavior?
If and when the next outbreak occurs, the same draconian and Orwellian measures that governments and corporations deployed in the name of combating COVID are still on the table.
And AI, Machine Learning, and the military will play an even bigger role than the last time around.
From analyzing wastewater to learning about disease spread; from developing pharmaceuticals to measuring the effects of lockdowns and vaccine passports, from modeling and predicting human behavior to coming up with messaging strategies to keep everyone in compliance — “improving preparedness for future public health emergencies” is becoming more militaristically algorithmic by the day.
“We are exploring innovative solutions to enhance our understanding of outbreak dynamics and to improve preparedness for future public health emergencies”
DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025
Why Isn’t There a Cure for Alzheimer’s Disease? A MIDWESTERN DOCTOR
Exposing the Great Amyloid Scam and The Cures They Buried for Billions
NOV 06, 2025
Story at a Glance:
• Alzheimer’s disease is commonly thought to result from abnormal plaque buildup in the brain that gradually destroys brain tissue.
•Almost all Alzheimer’s research for decades has been directed toward eliminating amyloid, even after the basis for much of this work was shown to stem from fraudulent research.
•The billions spent on amyloid Alzheimer’s research have only produced three drugs, all of which offer minuscule benefits and severe side effects.
•In contrast, affordable and straightforward treatments that reduce dementia or the preceding cognitive impairment have been maligned and buried by the medical industry.
•DMSO for example, has incredible neuroprotective qualities that have spared many stroke and spinal cord injury victims from a life of “incurable” disability. Decades of forgotten research also show it treats cognitive impairment and dementia.
•This article will review the great amyloid scam and the simple therapies for cognitive decline we’re never told about.
Medicine is strongly biased towards adopting biochemical models of disease as this facilitates costly therapeutics being developed for each disease and hence sustains the medical industry. Unfortunately, in many cases, the biochemical approach to disease, at best can manage symptoms, and as a result, many conditions remain “incurable” while non-patentable natural therapies that can cure them languish in obscurity.
That’s why, despite spending an ever increasing amount of money on Alzheimer’s research (e.g., the NIH spent 2.9 billion in 2020 and 3.9 billion in 2024), we’ve still failed to make any real progress on the disease. This is particularly remarkable given the vast costs to the country (e.g., last year Alzheimer’s was estimated to cost the United States 360 billion dollars) and the even greater social costs that accompany it.
The Amyloid Juggernaut
In 1906, plaques (of amyloid) in the brain were identified as the cause of Alzheimer’s disease. As the years have gone by, the majority of research for treating Alzheimer’s disease has been targeted at eliminating these plaques. Unfortunately, to quote a 2022 article:
Hundreds of clinical trials of amyloid-targeted therapies have yielded few glimmers of promise, however; only the underwhelming Aduhelm has gained FDA approval. Yet Aβ still dominates research and drug development. NIH spent about $1.6 billion on projects that mention amyloids in this fiscal year, about half its overall Alzheimer’s funding. Scientists who advance other potential Alzheimer’s causes, such as immune dysfunction or inflammation, complain they have been sidelined by the “amyloid mafia.” Forsayeth says the amyloid hypothesis became “the scientific equivalent of the Ptolemaic model of the Solar System,” in which the Sun and planets rotate around Earth.
Note: frequently, when a faulty paradigm fails to explain the disease it claims to address, rather than admit the paradigm is flawed, its adherents will label each conflicting piece of evidence as a paradox (e.g., the French “paradox” disproves the notion cholesterol causes heart disease4) and dig deeper and deeper until they can find something to continue propping up their ideology (e.g., cholesterol reducing statins provide almost no benefit for heart disease while having significant side effects yet continue being pushed on patients).
The consistent failure of the amyloid model to cure Alzheimer’s gradually invited increasing skepticism towards it, which resulted in more and more scientists studying alternative models of the disease. Before long, they found other factors played a far more significant role in causing the disease (e.g., chronic inflammation), and by 2006, this perspective appeared poised to change the direction of Alzheimer’s research.
In response, the amyloid proponents pivoted to defending their failed hypothesis was due not to amyloid clumps, bath rather toxic parts of it (oligomers) and a Nature 2006 paper appeared which identified a previously unknown toxic oligomer, Aβ*56, and provided proof that it caused dementia in rats.
This paper cemented both the amyloid beta and toxic oligomer hypotheses (as it provided the proof many adherents to the theory had been waiting for) and rapidly became one of the most cited works in the field of Alzheimer’s research. Its authors rose to academic stardom, produced further papers validating their initial hypothesis, and billions more were invested by both the NIH and the pharmaceutical industry in research of the amyloid and toxic oligomer hypothesis.
It should be noted that some were skeptical of their findings and likewise were unable to replicate this data, but rarely had a voice in the debate:
The spotty evidence that Aβ*56 plays a role in Alzheimer’s had [long] raised eyebrows. Wilcock has long doubted studies that claim to use “purified” Aβ*56. Such oligomers are notoriously unstable, converting to other oligomer types spontaneously. Multiple types can be present in a sample even after purification efforts, making it hard to say any cognitive effects are due to Aβ*56 alone, she notes—assuming it exists. In fact, Wilcock and others say, several labs have tried and failed to find Aβ*56, although few have published those findings. Journals are often uninterested in negative results, and researchers can be reluctant to contradict a famous investigator.
The Amyloid Scandal
At the end of 2021, a neuroscientist physician was hired by investors to evaluate an experimental Alzheimer’s drug and discovered signs that its data consisted of doctored Western Blots (and therefore erroneous assessments of what oligomers were present within research subjects’ brains). As he explored the topic further, he discovered other papers within the Alzheimer’s literature had been flagged for containing doctored Western Blots.
Note: Western blots, used to test for proteins, are one of the few easily detectable forms of research fraud (e.g., we discovered Pfizer submitted fake Western blots to regulators to “prove” their vaccine worked). Regrettably, far more undetectable fraud exists throughout the scientific literature (e.g., independent researchers comparing regulatory submissions discovered Pfizer also submitted doctored data on where the COVID vaccine is distributed in the body).
Before long, the neuroscientist noticed three of those suspect papers had been published by the same author and decided to investigate the author’s other publications. This led him to the seminal 2006 Alzheimer’s publication, which contained clear signs of fraud.
As investigation then uncovered 20 doctored papers written by the author, 10 of which pertained to Aβ*56 (along with a co-researcher attesting to earlier scientific misconduct by the author).
The Amyloid Industry
One of the remarkable things about this monumental fraud was how little was done about it. For example, the NIH was notified in January 2022, yet in May 2022, beyond nothing being done, the NIH gave the suspect researcher a coveted $764,792 research grant (signed off by another one of the authors of the 2006 paper).
In July 2022, Science published an article exposing the incident and the clear fraud that had occurred. Despite this, the researcher was allowed to remain in his position as a tenured medical school professor. It was not until June 2024 that the 2006 article was retracted at the request of the authors—all of whom denied being at fault and insisted the doctored images had not affected the article’s conclusions. Eventually, on January 29, 2025, during his confirmation hearing, RFK cited the paper as an example of the institutional fraud and wasted tax dollars within the NIH, and a few days later, the suspect researcher announced his resignation from the medical school professorship (while still maintaining his innocence).
This odd behavior (e.g., the medical field continues to insist the proven fraud has not disproven the Amyloid hypothesis) likely results from how much money is at stake—beyond the research dollars, roughly 7 million adults have Alzheimer’s—equating to hundreds of billions in potential (Medicare funded) sales each year.
The Failed Amyloid Drugs
Recently, a monoclonal antibody that made immune cells target amyloid demonstrated limited success in treating Alzheimer’s—which was embraced as revolutionary by the medical community, the pharmaceutical industry, and drug regulators. In turn, the first new drug received accelerated approval (which the FDA proudly announced). The second then received a quiet backdoor approval (due to the immense controversy surrounding the first), and the third was partially approved a year and a half later.
Each year, JP Morgan (Chase Bank) hosts a private conference for pharmaceutical investors that sets the tone for the entire industry. In 2023, its focus (covered in detail here) was on the incredible profitability of the new Alzheimer’s drugs and the GLP-1s like Ozempic (which the FDA has also relentlessly promoted). Most remarkably, the (widely viewed as corrupt) FDA commissioner was a keynote speaker, and a few days before the conference, had enacted the second backdoor approval.
However, despite the rosy pictures painted around the drugs (which each attacked different aspects of amyloids), they were highly controversial as:
• The FDA’s independent advisory panel, in a very unusual move, voted 10-0 (with one abstaining) against approving Aduhelm, the first amyloid drug (which targeted amyloid plaques), but the FDA approved it anyways. In a highly unprecedented move, three of the advisors then resigned, calling it “probably the worst drug approval decision in recent U.S. history.”
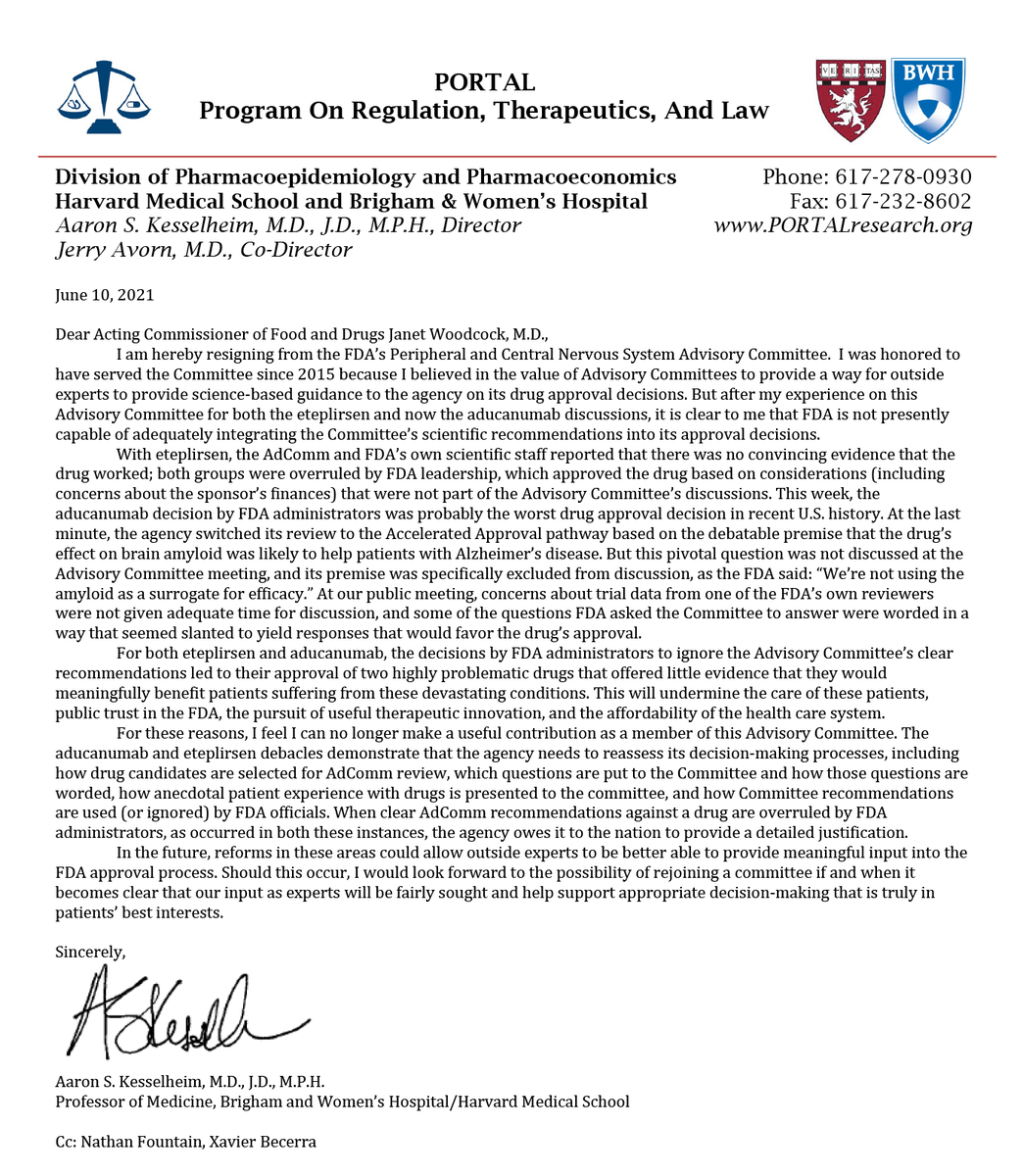{kind=link}
• That drug was priced at $56,000 a year—making it sufficient to bankrupt Medicare, (which attracted a Congressional investigation).
• Brain swelling or brain bleeding was found in 41% of patients enrolled in its studies. Additionally, headaches (including migraines and occipital neuralgia), falls, diarrhea, confusion, and delirium were also notably elevated compared to placebo.
• No improvement in Alzheimer’s was noted; rather one analysis found it slowed the progression of Alzheimer’s by 20% (although this could have been a protocol artifact rather than a real effect).
The second monoclonal antibody (which targeted amyloid precursors) had a somewhat better risk benefit profile (only 21% experienced brain bleeding and swelling due to reduced targeting of stable amyloid plaques), and 26.4% reduction in the progression of Alzheimer’s was detected in the trail (which for context, translated to a 0.45 reduction on a scale where a reduction of at least 1-2 points is needed to create an impact which is in anyway meaningful for a patient).
The third monoclonal (which targeted amyloid plaques thought to be more pathologic) was also contested as it caused 36.8% of recipients to develop brain bleeding or swelling, like the other amyloid medications, frequently caused headaches and infusion reactions (e.g., nausea, vomiting, changes in blood pressure, hypersensitive reactions or anaphylaxis) and there were reasons to suspect the trial had greatly overstated its minimal benefits.
Remarkably, despite widespread protest against the third drug, the FDA’s new advisory panel voted unanimously in favor of it, even though it had a very similar mechanism, efficacy, and toxicity to the previously unanimously rejected amyloid drug. It should therefore come as no surprise that, when the British Medical Journal conducted an independent investigation, it found that, within publicly available databases, 9 out of 9 (assessable) members of the advisory committee had significant financial conflicts of interest.
Fortunately, despite the aggressive promotion of amyloid drugs and the industry’s best attempts to promote the sector, the market somewhat recognized how bad they were. The first drug had its price halved (then was withdrawn as no one wanted it—making around 5 million dollars total), while the other two have had very modest sales (e.g., 290 million for the most popular one).
What Amyloids Drugs Show Us
From this, four things stand out:
• These drugs consistently damage brain tissue, indicating that their mechanism of action was inherently dangerous (e.g., it creates brain swelling by causing immune cells attacking amyloid also to attack brain tissue, or it creates brain bleeding by removing amyloid plaque that patches vessel walls and stabilizes brain tissue). Remarkably, despite this issue being recognized, it has not deterred the usage of these class drugs.
•Removing amyloid offers minimal benefit and may be counterproductive. In fact, one of the only protocols that has had proven success in treating Alzheimer’s instead views amyloid as a protective mechanism the brain uses to prevent further damage.
• An absolutely absurd amount of money and time has been wasted on this endeavor due to the medical field’s need to find a patentable drug.
•The focus on these lucrative drugs has diverted attention from other (off-patent) treatments that are more likely to help Alzheimer’s patients.
For example, a randomized controlled trial which gave MCTs derived from coconut found that over 6 months, 80% remained stable or improved—which for context, is better than what any of the amyloid drug trials showed, and more importantly, does not cause brain bleeds (and costs a lot less than the annual rough $30,000 cost for those drugs).
Note: numerous readers have shared that coconut oil improved their relative’s dementia.
Likewise, very few are aware of a 2022 study that should have revolutionized the entire Alzheimer’s field:

Note: the RECODE protocol was based around identifying the underlying cause of a patient’s cognitive impairment (as five different things can cause dementia), and then providing appropriate natural therapies to address the applicable cause. Since then, many others have replicated its success in their patients.
DMSO and Dementia
Dimethyl Sulfoxide (DMSO) is a naturally occurring compound that has a variety of unique healing properties that allow it to rescue tissues from dying and revive those damaged from previous injuries—best demonstrated by decades of evidence showing DMSO can heal strokes, brain bleeds, severe concussions, and spinal cord injuries and save patients from a lifetime of paralysis.
As many of DMSO’s mechanisms directly counteract the processes that trigger dementia, I have received many accounts like these from readers:
My uncle’s wife has dementia and has been unable to speak for over a year. My mom recently visited them and told them about DMSO. He began to give his wife DMSO orally. After two weeks she began to talk again.
I read the article and began giving it to my 93 year old mother in her juice every morning the end of November. She has had some form of dementia for over 15 years. Since taking the DMSO, she no longer suffers with severe sundowners. She is more “with it” and can communicate and laugh with us. Her personality is back. She is crossing her legs again and lifting her pinky finger when drinking her coffee. It’s a lot of little things that make a difference. She is able to understand when I am asking her to use the bathroom. She is more cognitive and has started coloring in her coloring books again.
I deeply appreciate your posts on DMSO. You helped bring spontaneous interaction back into the life of my father with Alzheimer’s.
Numerous studies support these experiences:
•When rats had their carotid arteries surgically modified to reduce the blood going to the brain, DMSO prevented both the neuronal damage and the significant loss of spatial memory and learning that otherwise occurred.
•In a similar study, rats who developed persistent and severe memory impairment from reduced brain blood flow received DMSO and FDP for 7 days, which improved their memory by 54%, nearly reaching the cognitive function rats whose blood flow was never cut off.1,2
•In rats, daily DMSO counteracted memory impairment induced by intracerebroventricular STZ infusions, while in a similar study, DMSO and Ginkgo biloba improved learning and memory in rats given Alzheimer’s disease.
•Drinking minute amounts of DMSO prevented the visual degeneration otherwise seen in rats engineered to have early Alzheimer’s disease. In another study of those rats, it protected key brain cells from disappearing and enhanced both their spatial memory and smell (while decreasing their anxiety). Likewise, in rats bred to develop cerebellar disorders, DMSO prevented age-related deterioration of certain cognitive functions (e.g., memory and spatial learning).
These results have also been replicated in humans:
•In 18 patients with probable Alzheimer’s after three months, DMSO greatly improved memory, concentration, and communication, alongside a significant decrease in disorientation in time and space.
•In 104 elderly adults with dementia due to cerebrovascular diseases, concussions, or Parkinson’s, DMSO combined with amino acids significantly improved their cognition and motor function.
•In 100 patients with cerebrovascular diseases (many of whom had dementia), DMSO caused almost all to have their cardiovascular parameters improve and:
“Recovery from the general symptoms was positive; there were favorable changes which were reflected in a feeling of well being, the recovery of agility, changes of mood from depressed to gay, improvement of sleeping, and clearer speech. As regards the ‘focal’ results, accelerated recovery from hemiplegia and hemiparesia was registered. A speedier recovery of speech in cases of defined or indicated aphasia took place.”
Note: I am currently sorting through all the existing DMSO literature (tens of thousands of papers) and am gradually discovering many other studies also showed DMSO can counteract severe neurological ailments like Alzheimer’s (e.g., one I found today discovered DMSO causes the amyloid precursor protein to be transformed into a form that protects rather than destroys neurons). Sadly, virtually all of these studies remain completely unknown (to the point I only found them through bulk DMSO searches) as the medical system has no incentive to ever promote therapies which cannot be profited off of.
Conclusion
The Alzheimer’s story illustrates how medical science’s relentless focus on commercializable products has failed the country. This must be replaced with prioritizing understanding the root causes of the chronic illnesses we face. If we do not do that and keep financially incentivizing the current lucrative paradigm, all we can expect is for health care to worsen and costs to reach increasingly unaffordable levels—best highlighted by the fact the government has now entered the longest shut down in history over disputes on continuing the costly 2016 ACA insurance subsidies (which had the net effect of more than doubling the cost of health insurance).
Note: I will be tuning into a hearing Senator Ron Johnson is holding on the “Affordable” Healthcare Act later today (which he highlighted the key points of here).
Fortunately, now that MAHA can set national health policy and independent media has broken the media’s monopoly over the truth due to the lies we saw throughout COVID-19, more and more are stepping outside the medical orthodoxy to pursue therapies that can actually heal them (and they can actually afford). An opportunity like this to unshackle ourselves from the medical monopoly has never existed before, and it is critical each of us brings attention to the need for real medicine before the window we have now to fundamentally change the practice of medicine closes.
Author’s note: This is a (reader requested) shortened version of a longer article which discusses the actual causes and treatments for Alzheimer’s disease. That article, along with additional links and references, can be read here. Additionally, a (recently updated) companion article on how DMSO treats neurological injuries (e.g., strokes, brain hemorrhages, traumatic brain injuries, spinal paralysis and developmental delay) can be read here.
Canadian Man Devastated After Government Euthanizes Both Grandmothers Frank Bergman
November 6, 2025
A Canadian man is sounding the alarm after both of his grandmothers were killed by government-sanctioned euthanasia within weeks in a double tragedy, he says has left deep wounds that will never fully heal.
“We’re here because two of my four grandparents died through euthanasia within two months of each other,” said Benjamin Turland, opening a powerful new video.
Turland told his story in the new short film released through Dying to Meet You, a storytelling project run by Amanda Achtman.
Achtman’s work has spotlighted Canadians who have been pressured into “choosing” euthanasia instead of receiving more expensive care.
Those featured include Roger Foley, who was repeatedly offered MAiD while seeking help, and Christine, an elderly woman who tattooed “Don’t Euthanize Me” on her arm out of fear of the system.
Turland’s testimony adds another devastating layer.
He described the moment his parents told him that his first grandmother had been euthanized under the government’s MAiD program:
“I’ve never had that experience before where I felt like someone punched me in the gut,” he said.
“She was most likely going to die within a few days by natural causes… it just wrecked me.”
Two months later, the grandmother he was closest to was also euthanized by the government.
She wasn’t just a family member; she was his confidant, his friend, even his roommate while he attended university.
They called each other “Bestie.”
Losing her by lethal injection left him questioning everything.
“There’s a strong guilt of like, why didn’t I say something?” he told Achtman.
“The message [her choice of euthanasia] sends to me is, I’m like, did I not love you enough?
“Did I not love you the correct way?
“Did I not make you feel like you are not a burden?”
The questions haunt him.
“If I could have had two more days with you, would I take that?” he said.
“Yes. Over anything.
“Because now I don’t have you…
“Even if you can’t talk… even if I just get to hold your hand.”
Slay the latest News for free!
We don’t spam! Read our privacy policy for more info.
For Turland, it wasn’t just the deaths; it was the method.
“It’s the choice of MAiD that hurts,” he said.
“With my grandfathers, I couldn’t have done anything about them passing…
“But when you choose it, I feel like there is something I could have done, and it impacts multiple generations.”
He pleaded with Canadians to talk openly with their elderly loved ones now, before they reach a vulnerable moment and feel pressured toward ending their lives.
According to Turland, these conversations may be difficult, but nothing compares to the pain of losing a grandparent through MAiD.
While supporters of euthanasia frame the procedure as compassionate relief, Turland says the reality is far more complicated: families are left confused, grieving, and wondering if they could have done more.
Activists, he noted, often tell them they aren’t “entitled” to their grief.
He rejects that entirely.
Life, he says, should be anchored in love and presence.
“You’re saying to them: I just want to be with you, for every moment, till every last breath,” he told Achtman.
“I don’t know why that would be a bad thing for them to hear, because they are going to feel so loved.”
As Canada prepares to expand euthanasia to include those with mental illness in 2027, stories like Turland’s are becoming increasingly urgent.
They serve as reminders that behind every MAiD statistic is a family left asking why.
READ MORE – Canadian Doctors Boast of Feeling ‘Energized’ After Euthanizing Patients
INSANITY: If Bovaer is killing cows in Denmark and causing cow miscarriages, what is it doing to the people drinking their milk? BRUCHA WEISBERGER
FDA admits “Bovaer is not for human use because it “may damage male fertility and reproductive organs..” yet allowed it for US cows despite 16.82% of administered Bovaer dose being excreted in milk.
NOV 06, 2025
BS”D
This is mind boggling. Bovaer is a drug developed to reduce cows’ methane output from their burps (yes, you read that right.) It has been misclassified as a “feed additive” in order to recklessly fast-track its approval process, despite studies showing it is carcinogenic and harmful to the reproductive system.
As of October, the Danish government forced farmers to add it to their cows’ feed, or face huge fines. The result? Many cows very sick, and some dead. Some cows miscarried. If 16.82% of the administered Bovaer dose is excreted in the cows’ milk, as the New Zealand toxicology study showed, what on earth is this drug doing to the pregnant women and children drinking the milk? What about the men, of whom the FDA said Bovaer may damage their fertility and reproductive organs?
Female rats were unable to become pregnant after exposure to the drug.
I wish I could say that this insanity has not reached the US yet – but Jon Fleetwood reports that “the U.S. Department of Agriculture awarded $22.8 million to Dairy Farmers of America to promote Bovaer use in California, Utah, and Idaho, and the product is already in use in Colorado, New Mexico, Kansas, Vermont, and New York.”
Please read Jon Fleetwood’s articles below and watch the video interviews of the devastated farmers on his original article link, if you can, or on the Danish journalist’s X handle (the videos are very important but I could not get them into my article here.)
I suggest you call the dairies that produce the milk you buy and tell them that you don’t want Bovaer in your milk.
A government-mandated “methane-reducing” feed additive called ‘Bovaer’ (here)—already linked to tumors, infertility, and residues in milk—has reportedly triggered a wave of catastrophic health problems in Danish dairy herds since its rollout on October 1, 2025.
Bovaer is developed by DSM-Firmenich (contact), which licenses the drug in Denmark directly.
Bovaer is licensed in the U.S. by Elanco (contact).
This website has been warning about Bovaer since December 2024 (here, here).
Farmers across Denmark are now reporting cows suffering from stomach cramps, fevers, miscarriages, sudden collapses, and drastic drops in milk production.
Some cows reportedly had to be euthanized.
Farmers say symptoms disappear when Bovaer is removed from the feed and return when it’s reintroduced—a pattern that’s prompted emergency calls for a government pause.
The reports are being documented by journalist Kent Nielsen on his Twitter/X account, @Kentfrihedniels.
You can see his X posts below.
Thinking of taking a flu shot? Read this first…
It’s not just that they’re ineffective, they also cause harm. Learn about safe alternatives such as Vitamin D, quercetin and zinc.
OCT 15, 2024 WORLD COUNCIL FOR HEALTH [Posted November 6, 2025]
If you’re of a certain age or demographic and in the northern hemisphere, chances are you’re being invited or encouraged to get a flu vaccine. The claim is that flu vaccines protect you and others from coming down with flu – and that if you do get it, the symptoms will be mild. So, is this true?
Many scientists see the flu shot as an unnecessary measure. For one thing, there’s a big question over whether the flu vaccine even works, particularly for older people, for whom it is recommended. Studies show that the vaccines often do not match the circulating viruses and no significant effects on serious complications or hospitalizations have been demonstrated.
You’d think that vaccinating people against flu would lead to a reduction in deaths from flu. But figures show that this isn’t the case. In fact, even though the number of flu shots given has increased more than eightfold, the number of flu-associated deaths has remained more or less unchanged.
There’s a logical explanation, and it goes like this:
Antibodies are not enough
Flu vaccines, like any other vaccine, primarily rely on the so-called Th2 antibody response. This generates antibodies to help the body fight off the influenza virus once it enters the bloodstream. What vaccines don’t do is impact the first line of defence in the nasal mucosa. This part of the innate immune system does not use antibodies, and it is here where respiratory viruses replicate.
This is why vaccines for respiratory viruses will never prevent infection or the transmission of the disease.
The immune response to vaccinations also decreases with age, which further reduces the already weak effect of vaccination in older people. Studies bear this out. In particular, a 2012 article in the British Medical Journal quoted an independent study that looked at data from 1967 to 2012 and concluded there isn’t strong evidence showing that the flu vaccine consistently protects people. While it does offer some protection for young, healthy adults who usually don’t face serious flu complications, the researchers noted that there is not enough evidence to support its effectiveness for older adults (65 and older), who account for more than 90% of flu-related deaths.
Recent research into the efficacy of flu shots also reveals their limitations
- In 2020, Anderson et al. showed that influenza vaccination of 60 to 70 year olds in England and Wales had no discernible positive impact on hospitalization or deaths:
- Another study in Japan reported on 83,146 individuals aged 65 years and followed them up over six years. In 2023, the incidence of hospitalization for influenza did not differ significantly by vaccination and the claimed protective effectiveness against incidence waned quickly after four or five months.
- Another 2020 study from Anderson and team analysed data covering 170 million episodes of care and 7.6 million deaths. Turning 65 was associated with a statistically and clinically significant increase in rate of seasonal influenza vaccination. However, no evidence indicated that vaccination reduced hospitalizations or mortality among elderly persons. The study points out that estimates were precise enough to rule out results from many previous studies.
This is not just a concern for the elderly but for all those with weakened immune systems, including those undergoing immunosuppressive treatments, or individuals with chronic health conditions. In such cases, the Th2 response may not produce enough protective antibodies to effectively combat the virus, leading to a higher risk of severe illness.
Here’s another reason to exercise caution of the flu vaccine:
Flu vaccines actually SPREAD the virus
Controlled studies published in the Proceedings of the National Academy of Sciences (PNAS) find that people who receive flu shots emit 630% more flu virus particles into the air compared to non-vaccinated people. In other words, flu vaccines spread the flu!
Physicians for Informed Consent has produced this concise summary of facts that you, your loved ones and your doctor should consider before a potential injection.
All this leads to an important next question:
If the flu shot isn’t a good idea, what is?
The flu shots’ limitations make the prevention and treatment of flu with nutritional supplements like Vitamin D, Quercetin, and Zinc more appealing and safe. These supplements not only enhance the immune response but also offer additional antiviral and anti-inflammatory benefits:
Vitamin D protects the lungs and airways – and much more besides
Studies have shown that Vitamin D supplementation can significantly reduce the risk of influenza infections by enhancing the body’s immune response. It works by modulating the expression of inflammatory cytokines and increasing macrophage function, which are essential for fighting off infections.
Moreover, Vitamin D has been found to protect the lungs and airways through the antimicrobial peptide cathelicidin, which has both antibacterial and antiviral properties. Vitamin D supplementation shows promise in reducing the risk and severity of respiratory infections, including influenza. The evidence suggests that consistent Vitamin D intake can lower the incidence of acute respiratory infections, shorten the duration of symptoms, and enhance immune response, particularly in the elderly. These benefits can translate into reduced hospitalizations and deaths due to flu, making Vitamin D a valuable component in flu prevention and management strategies.
Quercetin: a powerful antiviral and zinc’s vital wingman
Quercetin is a flavonoid found in many fruits and vegetables, known for its antiviral, anti-inflammatory, and antioxidant properties. It has been shown to inhibit the entry and replication of viruses in lung cells, making it a potent candidate for managing respiratory infections like the flu. Quercetin also acts as a zinc ionophore, facilitating the transport of zinc into cells, which enhances its antiviral effects. Studies suggest that the co-administration of Quercetin and Vitamin C can exert a synergistic antiviral action, further boosting immune response and reducing viral replication
Zinc: helps prevent and reduce infection severity and duration
Zinc is an essential mineral that supports various cellular functions of both the innate and adaptive immune systems. It interferes with the process that certain cold viruses use to multiply, thereby reducing the severity and duration of infections. Zinc is particularly important for the recruitment and activity of neutrophil granulocytes, natural killer cells, and T cells, all of which play critical roles in the immune response. Supplementation with zinc has been supported by evidence showing its effectiveness in preventing viral infections and reducing their severity.
In summary…
The questionable efficiency and safety of the flu vaccine raises important concerns that cannot be overlooked. Alternative approaches such as supplementing vitamin D, quercetin and zinc, are one way to enhance immunity without the risks associated with traditional vaccinations.
Moreover, the potential for the production of IgG4 antibodies as a response to the vaccine illustrates a complex interaction between immunization and immune system dynamics, where the very act of repeated vaccination may inadvertently lead to a weakened response against certain influenza strains. This effect can also result in the weakening of the immune system in general to fight infections and cancer. This highlights the need for continued research and dialogue about the benefits and risks of flu vaccination versus alternative preventive strategies.
As we navigate through flu seasons, it is crucial to remain informed and consider individualized approaches to immune health. Ultimately, a well-rounded strategy that includes lifestyle choices, nutritional support, and an understanding of the science behind flu immunization could empower individuals to make informed decisions that best suit their health needs. The World Council for Health stands for a better way.
References:
1. Berndt, Christina: ‘Experten mit den falschen Freunden’, http://www.sueddeutsche.de/wissen/staendige-impfkommission-experten-mit-den-falschen-freunden-1.271784. 49 Arbeitsgemeinschaft Influenza: ‘Was ist die AGI?’
2. http://influenza.rki.de/Arbeitsgemeinschaft.aspx. 50 Robert-Koch-Institut: Epidemiologisches Bulletin, 14.3.2011
3. http://www.gpk.de/downloadp/STIKO_2011_Bulletin10_110314_Schaetzung_der_Influenza_bedingten_Todesfaelle.pdf. 51 World Health Organization: »List of Members of, and Advisor to, the International Health Regulations (2005) Emergency
4. Committee concerning Influenza Pandemic (H1N1), 2009, http://www.who.int/ihr/emerg_comm_members_2009/en/index.html. 52 Jefferson, T.;
5. Di Pietrantonj, C.; Rivetti, A.; Bawazeer, G.A.; Al-Ansary, L.A.; Ferroni, E.: ‘Vaccines for preventing influenza in healthy adults’, in: Cochrane Database of Systematic Reviews, 2010, 7., Art. No.: CD001269, DOI: 10.1002/14651858.CD001269.pub4.
6. Wittig, Frank. Die weiße Mafia: Wie Ärzte und die Pharmaindustrie unsere Gesundheit aufs Spiel setzen, 2012Yan J, Grantham M, Pantelic J, Bueno de Mesquita PJ, Albert B, Liu F, Ehrman S, Milton DK; EMIT Consortium. Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Proc Natl Acad Sci U S A. 2018 Jan 30;115(5):1081-1086. doi: 10.1073/pnas.1716561115. Epub 2018 Jan 18. PMID: 29348203; PMCID: PMC5798362.
Covid injections pose risk of pilots having in-flight seizures even years after having taken a shot [11:25] BY RHODA WILSON
A couple of weeks ago, Dr. Kevin Stillwagon posted an update on pilot incapacitation. The Federal Aviation Administration does not maintain records of who took covid injections and when, he said.
But it gets worse, he said. “The FAA stopped entering data into the incapacitation data registry very early in the year 2021 and completely cancelled the program in 2022.”
“Trying to identify risks is even more critical now, because starting in December of 2020, airline pilots were forced to get injected with a product that causes subclinical myocarditis and has been tied to cerebrovascular events, including seizures, even several years after the injections.”
He concluded by issuing a call for pilots and other airline crew members to voluntarily have medical tests done to assess their risk of, for example. an in-flight seizure or cardiac event.
WATCH [11:25]