
COVID-19 / Malicious Medical Quackery
[Ed.: FEAR YOUR DOCTOR! Medicine is a disgraced profession. They cannot (and must not) be trusted any longer! Cultivate Nosocomephobia and iatrophobia. Spread ‘vaccine hesitancy’! How Bad is My Batch?]
[Ed.: If you know someone injured by the jabs, direct them to humanitysuit.com to become a plaintiff.]
[Ed.: How Bad is My Batch? Enter your batch number(s) and find out. Then take action and purge yourself of this shit to the extent possible. It’s do-able!]
Medscape Presents Long-COVID as Unassailable with Generic Drugs PETER A. MCCULLOUGH, MD, MPH
Patient Led Research Organization Fails to Cite Applications of Ivermectin, Colchicine, Hydroxychloroquine, and McCullough Protocol Base Spike Detoxification
DEC 13, 2024
Just as the public was misled during the acute phase of the SARS-CoV-2 outbreak with Medscape newsletters to doctors indicating no outpatient treatments were working, a similar dismal message hit the inboxes of America’s physicians in an article by Tinker Ready on long-COVID.
RSV Jab Halted by FDA for Infants 5-8 Months Old. How About All Others? ANDREAS OEHLER
Due to “imbalance” in safety signals.
DEC 12, 2024
As University of Minnesota reports on Dec. 11, 2024, “Pediatric RSV vaccine trials on hold, FDA says”:
A briefing document from the Food and Drug Administration (FDA) says that enrollment for all clinical studies of vaccines for respiratory syncytial virus (RSV) in infants is on hold over concerns about potential safety findings from a clinical trial involving two vaccine candidates.
The document, released ahead of a meeting tomorrow of the FDA’s Vaccine and Related Biologic Products Advisory Committee (VRBPAC), revealed that a phase 1 trial evaluating the safety, tolerability, and immunogenicity of two Moderna RSV vaccine candidates (mRNA-1365 and mRNA-1345) in infants aged 5 months to 8 months was paused in July after five cases of severe to very severe lower RSV respiratory tract infection (LRTI) were reported in infants who received a 15-microgram (μg) dose of mRNA-1345 (3 cases) or a 15-μg dose of mRNA-1365 (2 cases), compared with 1 case in the placebo group. 5 of the 6 infants required hospitalization, with 1 needing mechanical ventilation.
Visiting the referenced document, “Considerations for Respiratory Syncytial Virus (RSV) Vaccine Safety in Pediatric Populations” (FDA, 2024.12.12), we further learn the following details of these cases:
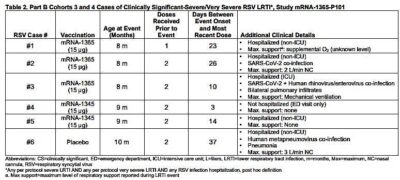
Basically, getting a jab “protecting” a baby from RSV gives the baby 500% higher odds of unfortunate severe RVS infection accompanied by coinfections within a month of the last jab (a series of 3!).
Nevertheless, the caring FDA approved three RSV jabs for 18+:
Abrysvo for active immunization for the prevention of LRTD caused by RSV in:
- individuals 60 years of age and older; and
- individuals 18 through 59 years of age who are at increased risk for LRTD caused by RSV
- Pregnant individuals at 32 through 36 weeks gestational age: Although not licensed for use in children, Abrysvo was approved on August 21, 2023, for active immunization of pregnant individuals at 32 through 36 weeks gestational age (GA) for the prevention of LRTD and sLRTD caused by RSV in infants from birth through 6 months of age. On September 22, 2023, the ACIP recommended Abrysvo for pregnant persons at 32-36 weeks GA using seasonal administration (meaning September-January in most of the U.S.) to prevent RSV-LRTD in infants <6 months of age (CDC, 2024a).
Arexvy for active immunization for the prevention of LRTD caused by RSV in:
- individuals 60 years of age and older; and Considerations for RSV Vaccine Safety in Pediatric Populations VRBPAC Briefing Document 9 of 39
- individuals 50 through 59 years of age who are at increased risk for LRTD caused by RSV
mResvia for active immunization for the prevention of LRTD caused by RSV in:
- individuals 60 years of age and older
Those 60+ seem to be able to withstand anything coming their way, FDA gathers. Or else, they must be disposed of on a priority basis?
Don’t we wish we were all deemed to be 5-8 months old!
What Makes Hospitals So Deadly and How Can We Fix It? Analysis by A Midwestern Doctor
1 Million Lives Lost – Who’s Really Behind the Curtain?
Lawsuits and whistleblowers reveal the devastating truth hospitals don’t want you to uncover. Is the system designed to harm instead of heal?
December 13, 2024
STORY AT-A-GLANCE
- Throughout COVID-19, abysmal hospital care and the suppression of effective off-patent therapies killed approximately a million Americans. Much of this originated from Obamacare pressuring hospitals to aggressively treat patients so they could quickly leave the hospital and reduce health care costs
- More frail patients respond poorly to aggressive protocols, resulting in them frequently being pushed into palliative care or hospice. Sadly doctors are no longer trained to gradually bring their patients back to health, and hence view many of those deaths as inevitable
- During COVID-19, hospitals enforced rigid protocols centered around remdesivir and ventilators while denying alternative treatments, even in cases where patients were likely to die — in one striking example, patients who received court-ordered ivermectin had a 95% survival rate compared to just 5% for those denied it
- Current medical training emphasizes following standardized protocols rather than practicing individualized medicine, with younger doctors being trained to execute procedures rather than critically examine cases and adjust treatment plans for each patient
- In this article, we will review some of the forgotten medical therapies that dramatically improve hospital outcomes and highlight some of the key strategies patients and lawmakers can use to reduce hospital deaths
During COVID-19, we witnessed something previously unimaginable. A national emergency hospitalized thousands of Americans, where they were cut off from their loved ones and inevitably died. It soon became clear that the hospital protocols did not work, but regardless of how futile conventional care was, patients in our hospitals could not get the alternative therapies they needed.
This led to a sobering realization throughout America — what many of us believed about our hospitals was utterly incorrect. Rather than help patients, hospitals effectively functioned like assembly lines that ran disastrous protocols (e.g., remdesivir), denied patients access to their loved ones and refused to use alternative therapies even when it was known the patients were otherwise expected to die.
This was best illustrated by a travel nurse who was assigned to the New York hospital with the highest death tolls in the nation and realized something very wrong was happening throughout the hospital so she covertly recorded it:
Watch [4:17]
Note: The full interview provides conclusive proof many patients were killed due to grossly inappropriate hospital protocols. A similar horrific testimony by another NYC COVID nurse can be viewed on my Twitter account here.
Appallingly, the COVID-19 treatment protocols financially incentivized remdesivir (“run death is near”) and then ventilator care but penalized effective off-patent treatments. As such, hospital administrators required deadly “treatments” like Remdesivir and retaliated against the doctors who used unprofitable treatments that saved lives.1
Note: The NIH continued to make remdesivir the treatment for COVID-19 and forbid alternative therapies even as a mountain of evidence piled up its protocols. This was due to Anthony Fauci appointing the NIH committee and selecting chairs that had direct financial ties to Remdesivir’s manufacturer — a recurring problem in American medicine (e.g., I showed how our grossly inaccurate cholesterol guidelines were authored by individuals taking money from statin manufacturers here).
Because of this murderous corruption, families began suing hospitals to allow the use of ivermectin for a relative who was expected to die (after being subjected to Fauci’s hospital COVID protocols). Remarkably, because there was so much money on the line, the hospitals chose to fight these lawsuits in court rather than just administer ivermectin.
Of the 80 lawsuits filed by lawyer Ralph Lorigo, in 40 the judge sided with the family, and in 40 with the hospital. Of those, in the 40 where patients received ivermectin, 38 survived, whereas of the 40 who did not, only 2 survived — in essence making suing a hospital arguably the most effective medical intervention in history. Yet rather than take this data into consideration, the profit-focused hospitals banded together to develop an effective apparatus to dismiss further lawsuits.2
As I had expected something like this to happen, shortly before the pandemic, I put a home treatment plain into place (e.g., by procuring high-powered oxygen concentrators and noninvasive ventilation). Numerous people in my immediate circle were successfully treated at home, many of whom would have otherwise been immediately hospitalized and likely died.
Note: Prior to COVID, we’d had other patients who merited hospitalization but simultaneously were likely to be put on the palliative care pipeline once admitted, so we’d already learned how to provide much of the care they needed at home.
Likewise, I also heard of more stories than I can count throughout the pandemic where a relative snuck an “unapproved” therapy to a patient in the hospital, saving the patient’s life.
Reductionist Realities
Every situation has two sides: the concrete factors and the intangible processes that lie between them. While modern science often focuses on optimizing the tangible, it tends to overlook the deeper essence of each phenomenon. However, those who nonetheless master these intangible aspects excel, as they solve a myriad of problems their peers cannot.
Leading Cardiologist: 100 Million Vaccinated Americans May Have IRREVERSIBLE Heart Damage By Frank Bergman
According to Dr. Thomas Levy, Covid vaccines are causing heart injury in at least 2.8% of people who receive the injections.
December 9, 2024
A leading cardiologist has warned that over 100 million Americans may now have irreversible heart damage after receiving Covid mRNA “vaccines.”
According to Dr. Thomas Levy, Covid vaccines are causing heart injury in at least 2.8% of people who receive the injections.
A minimum of 7 million Americans who took the Covid vaccine in 2021 now have severely damaged hearts, according to Dr. Levy.
However, the top doctor said that number is now likely to reach over 100 million people.
Dr. Levy is a renowned cardiologist and an attorney-at-law who also serves as the contributing editor for the Orthomolecular Medicine News Service.
Levy told MIT computer scientist and vaccine data expert Steve Kirsch that the spike protein’s effect on the heart is even worse than previously thought.
In an article, Kirsch, the founder of the Vaccine Safety Research Foundation (VSRF), highlighted the heart damage in vaccinated pilots.
As Slay News has previously reported, soaring heart damage among pilots was recently revealed in a change to Federal Aviation Administration (FAA) guidelines.
Back in 2022, the FAA quietly changed the electrocardiogram (ECG) parameters for pilots to accommodate those with cardiac injury.
The update suggests the injections are causing an unprecedented amount of pilots to fail their screening.
In its updated “Guide for Aviation Medical Examiners,” the FAA widened the ECG parameters beyond the normal range (PR max of 0.2).
According to Kirsch, this range wasn’t widened by a little, it was a lot.
“The cardiac harm of course is not limited to pilots,” Kirsch explained in his article.
“My best guess right now is that over 50 million Americans sustained some amount of heart damage from the shot.”
WATCH [1:29]
As Slay News recently reported, a major county in Washington state is battling a crisis of surging heart attack deaths among the almost universally Covid-vaccinated population.
King County, which covers Washington’s most populous city of Seattle, has a population of 2.271 million people.
A whopping 98% of King County residents received at least one shot of a Covid “vaccine” since they were rolled out for public use in early 2021.
However, an explosive study uncovered alarming data after analyzing autopsy records for the county.
The team of leading American researchers, led by world-renowned cardiologist Dr. Peter McCullough analyzed data for the county from 2015 to 2023.
The peer-reviewed study found a staggering 1,236% surge in excess heart attack and cardiac arrest deaths among King County’s residents.
Reflecting on this alarming data during an interview last week, Dr. McCullough said:
“So it looks like the vaccines are the smoking gun.”
The top doctor has been at the forefront of exposing the harms of the Covid mRNA injections.
In a separate interview last month, Dr. McCullough, one of the world’s most revered medical experts, issued a warning to the public that Covid mRNA “vaccines” were created to “strict military criteria” to serve as a “bioweapon.”
McCullough raised the alarm in a new interview while revealing the devastating impact on humanity caused by the mass global vaccination campaign.
“As a doctor, I have never seen something so injurious to the human body,” McCullough revealed.
The Covid “vaccines” are “a weapon,” he added.
“According to strict military criteria, it’s a bioweapon.”
WATCH [0:58]
Meanwhile, secret official data from Santa Clara County has exposed a shocking surge in all-cause deaths among residents who received Covid mRNA “vaccines.”
The spike in mortality rates was revealed in the county’s official statistics after the hidden records were unsealed by a Freedom of Information Act (FOIA) request.
The data shows that non-COVID-19 all-cause mortality (NCACM) started spiking during the first quarter of 2021 when the mRNA shots were first rolled out for public use.
Source: slaynews.com
Outgoing “Biden” Regime Extends PSYOP-19 ‘Emergency Declaration’ to Extend Legal Immunity to BigPharma DEATHVAX™ Manufacturers Until 2029 2ND SMARTEST GUY IN THE WORLD
DEC 12, 2024
The Modified mRNA slow kill bioweapon “vaccines” conveniently fall under this corrupt PREP Act, which provides sweeping liability immunity for vaccine manufacturers, distributors, licensed health professional and essentially anyone else that was pushing these deadly gene altering poisons, effectively preventing any and all lawsuits save for those considered “willful misconduct.” Of course, the entire scamdemic and associated “vaccines” fall under willful misconduct, and then some.
The illegitimate Federal government and its unconstitutional agencies are to this very day in late 2024 still pretending that COVID-19 is somehow an ongoing public emergency as they continue to stockpile like there’s no tomorrow these Emergency Use Authorization (EUA) spike protein factory injections; in other words, this is all for your protection and benefit, so that when (not if) you die prematurely from these “vaccines,” just remember that you saved granny, helped reverse “climate change,” and that your self-inflicted or voluntary euthanasia means that you are anything but an anti-vaxxer, anti-science domestic terrorist deplorable, such that upon precipitously departing this life you do so as a most virtuous virtue signaler.
Of course, Pfizer, Moderna, Fauci, Gates, et al. all thank you for your service.
The question now becomes, will Mister Operation Warp Speed aka President Trump finally admit the true nature of his “beautiful vaccines,” thus unleashing RFK Jr. et al. to reverse this PREP Act extension as they commence with the mass arrests of the bioterrorists that have further weaponized the Medical Industrial Complex on behalf of their Intelligence Industrial Complex handlers? Or will there be more of the same empty promises and blusterous patriotic rhetoric as more and more ‘new and improved’ Modified mRNA “vaccine” products are rolled out for followup scamdemics and other fake “health emergencies” in order to nudge the naive into continuing to partake in these statist mass bio-suicide rituals by subjecting themselves to these never-ending injections?
If the PREP Act is not overturned over the next couple of month, and if all of these BigPharma, NWO globopedo and Three-Letter Agency criminals continue to roam free, then you know exactly what MAGA and MAHA really stand for.
More shall be revealed imminently.
They want you dead.
Do NOT comply.
TERRIFYING: Hundreds Of Deadly Virus Samples That Can Be Weaponized Go Missing From Lab
December 11, 2024 Yeshiva World – In a shocking and deeply troubling biosecurity incident, health authorities in Queensland, Australia, have revealed that 323 vials of live viruses, including extremely lethal pathogens, are missing. Among the unaccounted samples are nearly 100 vials of Hendra virus, two vials of Hantavirus, and 223 vials of Lyssavirus, all of them lethal to humans. Despite their disappearance in 2021, the breach was only confirmed in August 2023, and only announced this week, leaving critical questions unanswered for over two years.
The breach occurred at Queensland’s Public Health Virology Laboratory when a freezer malfunctioned, forcing a transfer of the virus samples to another freezer. Alarmingly, proper documentation of the transfer was not completed. A health official added that while the samples may have been destroyed through routine autoclaving, the lack of records makes it impossible to verify their fate.
The missing viruses are highly dangerous and have the potential to cause devastating consequences:
- Hendra Virus: Known for infecting horses, this virus can jump to humans and has an alarming 57% mortality rate. It was first identified in Brisbane’s suburb of Hendra in 1994 and is naturally hosted by fruit bats.
- Hantavirus: Originating in rodents, this virus spreads through their droppings, urine, or saliva and causes Hantavirus Pulmonary Syndrome in humans, with a fatality rate of 38% in symptomatic cases.
- Lyssavirus: A rabies-like virus that is almost always fatal once symptoms appear, Lyssavirus claims an estimated 59,000 lives annually worldwide.
While officials have sought to reassure the public, their assurances do little to ease growing anxieties. Queensland Health Minister Tim Nicholls said there have been no recent cases of Hendra or Lyssavirus in Queensland and no recorded instances of Hantavirus in Australia. However, the delay in confirming the breach and the lack of clarity around the samples’ fate leave serious gaps in public confidence.
In light of this alarming breach, Queensland Health has commissioned an independent investigation. Retired Supreme Court Judge Martin Daubney AM KC and biosecurity expert Dr. Julian Druce will lead the inquiry to uncover how this failure occurred and establish measures to prevent future incidents.
Immediate steps have been taken to address systemic failures, including retraining staff, auditing permits, and reviewing storage protocols. “I want to stress that there have been no public health incidents linked to these materials,” Nicholls stated, though this reassurance may feel hollow given the scope of the breach.
Authorities have dismissed concerns of deliberate foul play, insisting there is no evidence that the samples were stolen or mishandled maliciously. Still, the fact that such lethal viruses could go missing highlights vulnerabilities in biosecurity practices.
“Vaccine Shedding”: Major Study Confirms Covid-Vaxxed Cause Side Effects in Unvaccinated People LIONESS OF JUDAH MINISTRY
The study finally confirms the existence of “vaccine shedding” – an issue previously shot down by health officials as a “conspiracy theory.”
DEC 11, 2024
By Frank Bergman December 10, 2024
A major new peer-reviewed study has confirmed that unvaccinated people can suffer from the harmful side effects of Covid mRNA “vaccines” by just being around people who have received the injections.
The study finally confirms the existence of “vaccine shedding” – an issue previously shot down by health officials as a “conspiracy theory.”
Alarmingly, the study found that unvaccinated people suffer vaccine harms even if they are “indirectly exposed” to those who received Covid mRNA shots.
A study titled, “Menstrual Abnormalities Strongly Associated with Proximity to COVID-19 Vaccinated Individuals,” was just published in the peer-reviewed International Journal of Vaccine Theory, Practice, and Research.
The team of top American researchers behind the study was led by Professor Jill Newman and Dr. Sue E. Peters.
The study revealed shocking findings: Unvaccinated women who were around vaccinated people daily (within 6 feet) suffered vaccine side effects.
The women suffered a 34% higher risk of heavy menstrual bleeding, a 28% higher chance of their period starting over a week early, and a 26% higher chance of menstrual bleeding lasting more than seven days.
Women with little close contact with vaccinated people saw no change.
One of the authors of the study wrote:
“After more than a year of censorship from the medical journals, our landmark study and manuscript have been published demonstrating significant circumstantial evidence that something is being shed from the COVID-19 vaccinated population to the unvaccinated population.
“It is far beyond time for these toxic injections to be withdrawn from the market.”
Reacting to the study’s alarming findings, esteemed physician Dr. Pierre Kory wrote on X:
“The most puzzling thing we’ve seen with the vaccine is its ability to ‘shed’ and harm those who never got it.
“A peer-reviewed study just validated the thousands of shedding reports sent to us.”
Dr. Kory also detailed the “vaccine shedding” phenomenon during an interview on American Thought Leaders.
WATCH [3:25]
In the study’s paper, the researchers prove the scientific plausibility of these findings by providing evidence supported by several key observations.
They discuss five key points in the paper:
Timing Consistency with Shedding Studies:
68.4% of respondents reported symptoms within one week of being near a vaccinated individual, with 48.6% experiencing symptoms within 3 days or the same day, aligning with the FDA’s guidance on vaccine-shedding timelines.
Prolonged Presence of Vaccine Components:
The detection of mRNA fragments and spike protein in vaccinated individuals’ blood for extended periods (up to 187 days) provides evidence of prolonged circulation of potential transmissible components.
FRIGHTENING: “Crystal-Like Fibers” Coming Out of a Person’s Fingers and Toes Following a Covid Injection LIONESS OF JUDAH MINISTRY
“…a woman named Margaret describes her granddaughter developing “crystal-like fibers” coming out of her toes and fingers following at least one COVID injection.”
DEC 10, 2024
Anybody aware of any stories like this one, describing “crystal-like fibers” coming out of a person’s fingers and toes following a COVID injection?
This interview was posted by Children’s Health Defense approximately a year ago. It features a woman named Margaret who describes her granddaughter developing “crystal-like fibers” coming out of her toes and fingers following at least one COVID injection.
“They’re clear. They’re crunchy. They’re long like a hair, and they’re in the cuticles of her toe. It then moved to all her fingers. And it was on her other toe also,” Margaret says. Margaret notes that she herself has had Morgellons before, and seems to speculate that it may be related?
For reference, according to Grok: “Morgellons disease (MD) is a condition characterized by a variety of symptoms, most notably the presence of fibers or filamentous structures under or emerging from the skin.” The disease apparently has an unknown etiology.
Grok also notes that a “2012 study by the Centers for Disease Control and Prevention concluded that the condition was similar to delusional infestation, with fibers primarily identified as textile material. They did not find evidence of a new infection or a common identifiable medical condition.”
Science Confirms Sv40 DNA in Pfizer’s Covid Shot, Validating Concerns Over Unexplored Genetic Health Risks [VIDEO 15:40] LIONESS OF JUDAH MINISTRY
A recent peer-reviewed study led by three German researchers has confirmed the presence of significant amounts of residual DNA, including the controversial SV40 promoter, in Pfizer’s COVID-19 vaccine
DEC 10, 2024
By Tamara Ugolini December 09, 2024
The peer-reviewed findings confirm the presence of significant residual DNA, including the controversial SV40 promoter, in Pfizer’s COVID-19 vaccine, igniting further concern around the long-term risks, transmissibility, and potential gene therapy implications that regulators fail to address.
A recent peer-reviewed study led by three German researchers has confirmed the presence of significant amounts of residual DNA, including the controversial SV40 promoter, in Pfizer’s COVID-19 vaccine vials.
Titled “BioNTech RNA-Based COVID-19 Injections Contain Large Amounts Of Residual DNA Including An SV40 Promoter/ Enhancer Sequence,” the findings validate previous research by genomics expert Kevin McKernan and virologist David Speicher, and further authenticates the concerns of people like former pharmacist specializing in regulatory oversight Maria Gutschi, molecular biologist Laura Braden, pediatric neurologist Eric Payne, biochemist Jessica Rose and more.
The findings directly contradict what infectious disease researcher Tara Moriarty told CUPE union members in September 2021 during a vaccine policy town hall where “vaccine hesitant” members had their concerns quelled through blatant misinformation by the supposed expert.
McKernan broke down the findings of the recently published study, raising serious concerns for public health with unprecedented, unregulated, and uncontrolled risks associated with these novel, modified RNA spike protein injections.
He calls the recent research “the final nail in the coffin” that confirms the presence of DNA, in disturbing amounts that are often three or fourfold higher than regulators have deemed ‘acceptable.’
McKernan points to another paper showing that the DNA amounts found in these vials are likely underestimated, with only 30% of the DNA being detected in standard analyses, suggesting the true amount of DNA in the vials could be as high as 100 to 140 nanograms (ng) – magnitudes higher than the FDA and WHO’s 10 ng/dose threshold.
Despite this research, and others confirming that DNA from vaccines is entering the bloodstream of individuals injected with mRNA, contamination continues with regulators failing to effectively address the potential repercussions.
Ian Brighthope: “60 million deadly vaccines have been administered” [2:14]
The heartbreaking moment when Professor Ian Brighthope breaks down in tears in front of thousands of people in Perth upon realizing that 60 million deadly vaccines have been administered to innocent Australians, now causing death and cancer.
Newly Published Study Shows Shedding Of Covid mRNA Vaccine Products PIERRE KORY, MD, MPA
A new study found a strong association of new onset menstrual irregularities with “indirect” exposure to Covid vaccines, i.e. being in proximity with vaccinated persons. Shedding is real.
DEC 09, 2024 – As many of my readers know, about a year ago I spent months researching and writing on the topic of “shedding” of gene therapy medicinal products (GTMP), a class of therapies which the Covid vaccines are categorized under. That effort was first inspired by patients reporting to me and my partner Scott Marsland at our vaccine injury/Long Covid Leading Edge Clinic that new and chronic symptoms were flaring after social outings and/or close exposures to recently vaccinated individuals.
A classic example from one of my patients: “Hey Doc, every time I go to Trader Joes, I feel terrible because all of my symptoms flare up and I have to get out of there within 10 minutes, why is that?”
Before I go on, I want to remind all of the prescience of the founder of the private Centner Academy in Miami, Leila Centner. In early 2021, out of concern for shedding exposure to the spike protein, she prohibited students from attending the school within 30 days of vaccination (which admittedly was a guess as to how long shedding might occur after vaccination):
Bird Flu: The “Next Pandemic” Is Right On Schedule 2ND SMARTEST GUY IN THE WORLD
DEC 09, 2024 – As the slow kill bioweapon-induced VAIDS epidemic gains momentum, and as the powers that be work overtime to foment various psyops and false flag events to thwart President Trump’s second term, what we are now witnessing is that PSYOP-25 may very well be on deck as their next disruptive scheme.
Fauci’s henchman Peter Hotez was recently activated in a predictive programming strategy to normalize their followup scamdemic exactly as his demented boss had done in 2017 in order to subvert President Trump’s first term:
Hotez, who over the last several decades was “awarded” grants in the tens if not hundreds of millions of dollars to come up with a vaccine for hookworm with exactly nothing to show for his “research” to date, is somehow still “expert” enough to now be warning of “big picture stuff coming down the pike starting on January 21st” like bird flu, more coronaviruses, SARS Mosquito-transmitted viruses, Dengue, Zika, Oropouche virus, yellow fever, whooping cough, measles and even polio, or all of his gain of function and vaccine-induced diseases.
The only big picture stuff that should be coming down the pike on January 21st are mass arrests of these bioterrorist sociopaths:
[Ed.:
Was DoD the Managing Agency for Operation Warp Speed? ROBERT W MALONE MD, MS
Pfizer did not commit fraud, but rather delivered the fraud that the US Government ordered
DEC 08, 2024 – Quite a bit of controversy has been generated by those who assert that the Pfizer contract issued by the DoD for the Bio N Tech mRNA COVID “vaccines” proves that the DoD was the managing agency for the development of this product. The phrase “Pfizer did not commit fraud, but rather delivered the fraud that the US Government ordered” certainly has more than a grain of truth. In contrast, my understanding and analysis indicates that the leading proponents of the theory that this contract proves that DoD was the agency that managed operation warp speed appear to not have a full appreciation of the nuances, and have overstated the implications. The purpose of this essay is to help the general public to gain more insight into the back story of this non-Federal Acquisition Regulations contract, which employed a non-traditional federal contracting vehicle known as an “Other Transactional Authority” contract.
If you really want to understand how the sausage gets made within the US Government with these big programs, I hope you will stick through this essay to the end.
Unfortunately, the two leading proponents of this theory of the case (Watt and Latypova) have seen fit to repeatedly personally attack both myself and my wife Dr. Jill Malone for years now as part of their advocacy of this interpretation, presumably because of my long history of working with the US Department of Defense in the Biodefense sector, and in particular with the Defense Threat Reduction Agency Chemical and Biological Technologies Directorate (DTRA CB), which is “dual-hatted” as the Joint Science and Technology Office for Chemical and Biological Defense (JSTO-CBD) under the Department of Defense Chemical and Biological Defense Program (CBDP).
Some Relevant Bona Fides
Those who have followed me closely may recall that over two years ago I was the first to disclose that a different branch of DTRA, the Threat Mitigation Branch (based on Fort Belvoir, VA), was a major funder of the Chinese CCP/PLA Wuhan Institute of Virology, and so shared responsibility with NIH/NIAID for the funding which lead to the eventual release of SARS-CoV-2 into the world. The DTRA/Threat Mitigation Branch funding was provided in the context of the DTRA/TMB “International Cooperation” activities, which are focused on cooperative threat reduction. DTRA CB chain of command is separate from DTRA/TMB at the level I was interacting with them, and I had no knowledge of the WIV funding until I started asking questions of DTRA GS employees that I knew when it became clear that there had been USG funding of the WIV.
The DTRA Threat Mitigation Branch is headquartered at Fort Belvoir, Virginia, and has personnel stationed at various locations worldwide. The branch is organized into several teams, including:
- Research and Development: Conducts research and development in areas such as blast effects mitigation, counter-CBRN agents, and non-lethal effects.
- Threat Analysis and Forecasting: Analyzes and forecasts emerging threats, providing strategic insights to inform DTRA’s counter-WMD efforts.
- International Cooperation: Collaborates with international partners to reduce the threat posed by WMD and related materials, technologies, and expertise.
- Operations and Training: Develops and conducts training exercises, and provides operational support for DTRA’s counter-WMD efforts.
Budget and Funding
The DTRA Threat Mitigation Branch receives funding through the Department of Defense (DoD) budget, with a focus on research and development, operations, and international cooperation. The branch’s budget is allocated across various programs and initiatives, including blast effects mitigation, counter-CBRN agents, non-lethal effects, and cooperative threat reduction.
One of the DTRA CB / JPEO CBD programs for which I served as a contractor was named “DOMANE,” and was envisioned and managed by Dr. David Hone, a GS-15 level government employee (GS-15 is basically the same rank as a brigadier general.) Dr. Hone and I came up with the concept of DOMANE during a discussion at my horse farm, but Hone developed and managed the program. Another character in this sordid affair who has written thousands of hate posts about me is George Webb, who repeatedly and ignorantly asserts that I was the director of DOMANE- as if a part-time contractor would be assigned to run a major DTRA CB drug discovery and repurposing program. At one point, in some web-based DOMANE communication, it was asserted that DOMANE should get credit for the development of Remdesivir- consequent to DTRA CB funding for the (failed) African clinical trials that tested use of Remdesivir for treating Ebola infection. On the basis of this, there emerged a cluster of haters (lead by George Webb) that assert that I was responsible for Remdesivir being approved for COVID. Just to say it, neither myself nor (to the best of my knowledge) DTRA-CB or the DOMANE program had any role in advancing Remdesivir for use to treat COVID. I understand that NIH/NIAID and Dr. Anthony Fauci, specifically, were responsible for this travesty, not DTRA CB, and certainly not me.
What is an OTA?
The notorious DoD Pfizer contract that Watt and Latypova often speak of was issued under a special federal contracting process known as an “Other Transactional Authority” or OTA. The OTA structure was put into place in response to general governmental bureaucratic frustration relating to biodefense product development and acquisition under the standard contracting process that is subject to the Federal Acquisition Regulations or FAR. The FAR is written to cover all Federal acquisition activities – from developing and purchasing pencils to tanks, planes, submarines, and aircraft carriers. As you might imagine, the FAR is extraordinarily detailed and cumbersome. The process of issuing and awarding a FAR-compliant contract can take up to two years, often at least nine months if very actively expedited. And, as one might hope, it requires many legally binding commitments from the contractor (the company getting the contract from USG). For example, these typically include keeping daily time sheets for all company employees – including those in management or not actually working on the contract! A company that fails to fulfill USG contract obligations under a FAR-compliant contract can be placed under terms that require it to pay back the full contract to the government, and even to pay for a competitor to perform the task or deliver the product to the government. The contracting instrument for this is called a “cure letter”. I have had three clients during my career that had been placed under cure letters – not due to any fault of mine – and I can attest that this is a major big deal. Issuing and managing/overseeing/auditing FAR-compliant awards is very labor-intensive for the USG.
There are two major issues that the USG has to contend with concerning large FAR-compliant contracts. First, the pool of trained and certified contracting officers (CO) is getting smaller and smaller. Becoming a CO is a high-risk pathway for a government employee. As part of their training, it is made clear that CO will go to jail if evidence of contracting corruption or malfeasance is identified. No glory, modest pay, and lots of risk and responsibility. Not something that many govies want to take on. The contracting officer corps has been retiring out for many years now, diminishing from year to year. Second, corporations (often referred to as “beltway bandits”) that specialize in federal contracting are usually not leaders in technology (or drug) development, and those who are leaders are focused on their sector and not on federal contracting. To illustrate the point, it has been my experience over decades that a federal FAR-compliant contract will add about 30% to 50% overhead to the cost of doing the work for a private sector contract. So, if you are a big pharma or biotech innovator, you have to be pretty desperate to want to work for the US Government.
What’s a government agency to do? Particularly one tasked with rapidly developing medical countermeasures to engineered pathogens and emerging infectious diseases?
Well, the developed answer was the Other Transactional Authority or OTA. Basically the idea here was to develop a compromise. By limiting the scope to just research and development of a “solution” through to a “demonstration” product (rather than actually acquiring the “solution” or “product,”) a simplified contract could be rapidly developed and issued, and the more burdensome contracting clauses could be waived without breaching the FAR, which was designed for actual acquisition and deployment. And to make this system run even faster, it was decided that contractors could be “pre-qualified” as suitable for award of an OTA by making them pay a fee to a private company that would vet their suitability – and in this way circumvent some of the problems with the diminishing CO staffing issue. In other words, outsource many of the contracting officer tasks to the private sector. The way this actually works is that the company that wants to get federal OTA contracts has to pay a fee to the outsourced private contracting company to pre-qualify them. Sort of like having to pay your bank to pre-qualify you for a home loan if you want to get a house financed.
Here is an AI-generated summary of how this works for the DoD:
CATASTROPHIC BOMBSHELL: First Ever Definitive Proof That Pfizer’s COVID “Vaccine” Integrates Into The Human Genome 2ND SMARTEST GUY IN THE WORLD
DEC 06, 2024 – The genetic sequence found in Pfizer’s Modified mRNA slow kill bioweapon “vaccine” integrates into the human genome, and now all future “vaccinated” generations are genetically modified , as well as their offspring.
These Pfizer genetic sequences will be passed on forever in not just the “vaccinated,” but, also, in the offspring of unvaccinated individuals procreating with those that have been genetically modified.
And now, for the first time ever, it has been irrefutably proven that DNA contamination from these “vaccines” is not some accidental “contamination” or benign artifact, but, rather, a ticking time bomb that will permanently alter the genetic fabric of humanity.
We have evidence that the SV40 promotor sequences that were deliberately added to Pfizer’s deadly “vaccine” are aggressively replicating inside the very tumors that they are causing, thus accelerating the metastization of VAIDS-induced turbo cancers; to wit:
A Cure to Long Covid & Vaccine Injury Syndromes. JOHN LEAKE
Dr. Peter McCullough’s new paper, published by the European Society of Medicine, just set the standard of care for this great scourge of our time.
DEC 04, 2024
In case you missed it or didn’t quite catch its significance due to the Latinisms in the title, my colleague Nicolas Hulscher just announced on our Substack that Dr. Peter McCullough has—through tireless investigative scholarship and clinical practice—honed in on a cure for Long Covid & Vaccine Injury Syndromes.
Before I go into the details of Nic’s triumphant announcement, I’d like to give a bit of background information about what we believe is the primary cause of Long Covid & Vaccine Injury Syndromes—namely, the Spike Protein.
There is a steadily increasing body of evidence that the spike protein of SARS-CoV-2 and the spike protein induced by COVID-19 mRNA vaccines linger in the body for an indeterminate period of time.
Long Covid Syndrome and Vaccine Injury Syndrome seem to be closely related and to amplify each other. Because the vaccine does NOT prevent infection, we have seen cases in which the patient is repeatedly exposed to the viral spike protein and the spike protein induced by the vaccine and boosters. Moreover, we are concerned that the vaccine may actually be impairing the immune system’s ability to mount an effective response when it is exposed to new variants. The trouble with the viral spike protein seems to be related to the fact that it did not arise through natural evolution, but was optimized in a laboratory to infect humans.
Thus, the key to treating both Long Covid and Vaccine Injury Syndromes is eliminating the foreign spike protein from the body. The clearest clinical expression of this syndrome is COVID-19 vaccine-induced myopericarditis, which even the CDC has acknowledged (while deceptively obscuring the true prevalence of this debilitating side effect).
For the last three years, Dr. Peter McCullough has tirelessly sought to find any safe and effective molecule or combination of molecules that could eliminate the spike. While no silver bullet—such as penicillin against syphilis—has been found, he has assembled Spike detoxification protocol, consisting of over-the-counter Nattokinase, Bromelain, and Curcumin. For patients suffering from Myopericarditis, colchicine is added to the protocol.
As Nic Hulscher just announced this morning, the paper titled Resolution of Refractory COVID-19 Vaccine-Induced Myopericarditis with Adjunctive Rapamycin—co-authored by Nicolas Hulscher, Dr. Peter McCullough, and Alexander Vickery—has just been published by the European Society of Medicine. As they noted in their Abstract:
COVID-19 vaccine-induced myopericarditis is now commonly encountered in clinical practice. The mainstay of clinical management involves vaccine Spike protein detoxification and colchicine for 12 months or longer. Herein, we present a case of a previously healthy 23-year-old male with autism spectrum disorder who developed COVID-19 vaccine-induced myopericarditis and class II heart failure. He was treated with Spike detoxification**, which is the combined use of over-the-counter nattokinase, bromelain, and curcumin, in addition to colchicine. [Emphasis added] While transient heart failure resolved, his chest discomfort persisted and at times was debilitating. Serial electrocardiograms indicated persistent global ST segment elevation. We describe the successful addition of off-label oral rapamycin to arrest inflammatory processes, extirpate ST elevation, and significantly improve quality of life. We summarize existing research that provided a rationale for the use of rapamycin. Concisely, these include targeting autophagy, mRNA translation, and immune activity modulation. We propose that mTOR inhibitors should be investigated as a potential disease-modifying interim treatment for COVID-19 vaccine induced cardiac injury.
Note that rapamycin is a macrolide compound derived from the bacterium Streptomyces hygroscopicus that was isolated for the first time in 1972, from samples of Streptomyces hygroscopicus found on Easter Island.
Rapamycin is used to coat coronary stents, prevent organ transplant rejection, treat a rare lung disease called lymphangioleiomyomatosis, and treat perivascular epithelioid cell tumour. It has immunosuppressant functions and is especially useful in preventing the rejection of kidney transplants.
With this paper entering the peer-reviewed literature, Dr. McCullough and his colleagues have just set the standard of care for this great scourge of our time.
Readers who wish to delve deeper into the details of the McCullough detoxification protocol and this new paper are encouraged to read Nicolas Hulscher’s post of this morning: BREAKING – New Peer-Reviewed Study: Resolution of Refractory COVID-19 Vaccine-Induced Myopericarditis with Adjunctive Rapamycin
I hope the Nobel Committee will be apprised of this development and grasp its significance, though I’m not holding my breath.
** [Ed.: Here is my spike protein detox regimen:
Nattokinase https://is.gd/pwPReU 240 caps $13.99
Lumbrokinase (30x more powerful than nattokinase) https://is.gd/M1D5bk 120 caps $17.95
Curamin Extra Strength (TM) (100% bioavailable turmeric) https://is.gd/i6dOVI 120 tabs $70.05
Bromelain https://is.gd/ZILADO 2,000 mg 240 caps $17.05
Dandelion Root Extract https://is.gd/fR0PMT 2 fl. oz $9.99 $129.03
Dr. McCullough’s protocol: 120 Caps $89.99
Selenium 75 mcg
Tumeric root extract 500 mg
Bromelain 500 mg
Nattokinase 400 mg
Black Seed Extract 100 mg
Dandelion root extract 50 mg
Black pepper root extract 5 mg
A new paper confirms presence of DNA in COVID-19 shot vials, settles issues pertaining to DNA quantification methods, shows spike persistence and exosomal shuttling JESSICA ROSE
And this was done in human cells…
DEC 04, 2024
Ulrike Kämmerer, Verena Schulz and Klaus Steger have just published what might be the paper of the century entitled: “BioNTech RNA-Based COVID-19 Injections Contain Large Amounts Of Residual DNA Including An SV40 Promoter/Enhancer Sequence”. It got through peer review on December 3, 2024 and it confirms much of what has already been evidenced and answers many questions lingering in the background.
Let’s unpack their results:
We demonstrate successful transfection of nucleoside-modified mRNA (modRNA) biologicals into HEK293 cells and show robust levels of spike proteins over several days of cell culture. Secretion into cell supernatants occurred predominantly via extracellular vesicles enriched for exosome markers. We further analyzed RNA and DNA contents of these vials and identified large amounts of DNA after RNase A digestion in all lots with concentrations ranging from 32.7 ng to 43.4 ng per clinical dose. This far exceeds the maximal acceptable concentration of 10 ng per clinical dose that has been set by international regulatory authorities. Gene analyses with selected PCR primer pairs proved that residual DNA represents not only fragments of the DNA matrices coding for the spike gene, but of all genes from the plasmid including the SV40 promoter/enhancer and the antibiotic resistance gene.
Spike protein expression in HEK293 cells after transfection with BNT162b2 biologicals is seen in green. This means the LNPs dump their payload successfully into human cells and this payload is translated into spike protein using the cell’s machinery (ribosomes) as per the design. The spike had a cytotoxic effect on cells (bad for cells = they die) and stuck around for at least 7 days (persistence). And that’s just when they stopped measuring. Spike got into the medium that the cells were in: it was released from the cells that were transfected. Spike can be cleaved from the membranes of cells, but, can also be exported in exosomes in full form (uncleaved).
This is an incredibly important finding and has massive implications for shedding. Exosomes – which are like little information carriers between cells – are likely trafficking/shuttling spike to other cells in the in vivo setting. Based on these findings, there’s no reason to believe they wouldn’t be doing this.
The amount of RNA in the injected Pfizer product (30 ug) checks out. The “real” amount of DNA that they found after additionally treating with RNase to remove interfering signals from RNA exceeded EMA limits by 4-5 times.
How to talk to mRNA fanatics ALEX BERENSON
Someone I know who got vaccinated and regrets it is stuck arguing about Covid jabs with people in his (very woke) workplace. He asked for help. Here’s what I told him.
DEC 03, 2024
Hard-core Covid vaccine advocates haven’t given up yet.
Fewer Americans are receiving mRNA boosters this fall than ever before. In Washington state, jabs are down about 25 percent from 2023. In red states, Covid shots barely exist anymore. Barely 5 percent of Floridians have had a 2024 booster.
Still, mRNA fanatics won’t quit. Even if they aren’t getting jabbed , they insist the shots worked as advertised. And they always – always – rely on The Chart. A person I know who initially trusted the jabs but has since seen the light asked me for help in a fight over The Chart this week.
You know The Chart. I’m not going to post it here, but it purportedly shows much higher death Covid rates among the unvaccinated than the jabbed throughout 2021. (The Chart NEVER shows raw numbers of deaths, just rates.)
Look at The Chart! the believers say. The Chart is Science with a capital S. The Chart is Numbers with a capital N.
You can’t argue with The Chart!
Well, yes, you can. The Chart is badly flawed because of a problem in epidemiology called “healthy vaccinee bias.” (More about healthy vaccinee bias here.1)
But mentioning healthy vaccinee bias can be frustrating. It requires some knowledge of the papers that discuss it. (Prove it! Oh, you can’t!) It’s fighting about data at a granular level.
Worst of all, it sounds like an excuse.
I wanted to offer a different way to debate The Chart.
A more holistic approach, if you like. It concedes some ground to the fanatics without giving up the key issue. It’s short and punchy and, I hope, relatively easy to follow – 14 texts, plus one chart, of Covid deaths from Vermont, which you can find here (down the linked page). Yep, the fanatics have a chart, now skeptics have a chart too.
Best of all, it’s true.
Here goes:
[Ed.:

Massive Spike Protein Pathogenicity Research Library Published NICOLAS HULSCHER, MPH
Over 250 peer-reviewed scientific studies confirm that the Spike protein is highly pathogenic on its own.
DEC 03, 2024
A comprehensive list of over 250 peer-reviewed studies demonstrating SARS-CoV-2 Spike protein harms has just been published by Erik Sass and Dr. Martin Wucher: SARS-CoV-2 Spike Protein Pathogenicity Research Library
This enormous body of research demonstrating that Spike protein is a highly toxic substance confirms that the COVID-19 injectable products are fundamentally unsafe for human use. Moreover, these data further amplify the rationale for Spike protein detoxification:
Much of academia and our public health authorities continue to ignore Spike protein as a target for long-COVID treatments. Last week, Medscape published an article titled, New Data: The Most Promising Treatments for Long COVID, where there’s not a single mention of the highly persistent Spike protein that has been identified in autopsy and biopsy findings of injured and deceased individuals.
The new U.S. administration should allocate funding to investigate accessible methods for detecting Spike protein and initiate large, prospective, double-blind, placebo-controlled trials to identify safe and effective treatments for removing Spike protein from the body, with endpoints including the clearance of Spike protein, improvement in inflammatory markers, and measurable symptom relief.
Nicolas Hulscher, MPH
Epidemiologist and Foundation Administrator, McCullough Foundation
www.mcculloughfnd.org
Please consider following the McCullough Foundation and Nicolas Hulscher on X (formerly Twitter) for further content.
A German lab has started to offer tests for “vaccine” spike proteins and plasmid DNA to those who suspect they have been injured by covid “vaccines” SUPER SPREADER
The purpose of the tests is to allow people who believe they have been injured by a covid “vaccine” to present evidence in court. [Expose-news]
DEC 03, 2024
The Institute of Molecular Diagnostics (Inmodia GmbH) is offering tests to establish whether a person’s body has vaccine spike protein or DNA plasmids. The purpose of the tests is to allow people who believe they have been injured by a covid “vaccine” to present evidence in court, for example, to support their claims. Additionally, the tests will help collect evidence to support the argument for discontinuing the use of covid injections.
By Rhoda Wilson on December 3, 2024
The following information is according to Inmodia’s website.
Never before in the history of medicine has a vaccination been associated with such a high number of serious side effects and consequential harm, including deaths occurring simultaneously. This situation arises primarily because the covid-19 vaccine is not a vaccine as we know it but rather a novel gene-based product that utilises an untested technology in humans.
Two different forms of genetically engineered injections were used in the global covid vaccination campaign. In both cases, the injections forced our bodies’ cells to produce the foreign spike protein (SARS-CoV-2, Wuhan variant).
In the case of DNA-based injections (AstraZeneca, Janssen / Johnson & Johnson), the blueprint for the spike protein is available in the form of a DNA copy, which is introduced into the cells with the help of an adenovirus envelope. Once inside the cell, the DNA must first be transcribed into mRNA.
In the case of RNA-based injections (Pfizer-BioNTech, Moderna), the blueprint for the spike protein, which occurs naturally on the surface of coronavirus particles, is already available as mRNA, which is introduced into the cells with the help of an envelope of partly synthetic fat-like molecules (lipid nanoparticles, LNPs).
This “vaccine mRNA” is not natural but genetically modified (“modRNA”). The chemical composition of the modRNA has been modified by Pfizer-BioNTech and Moderna in many ways so that the end product no longer corresponds to a naturally occurring mRNA. The modRNA has a significantly extended lifespan and therefore leads to a maximum and long-lasting production of exogenous spike protein.
modRNA is synthesised based on a DNA template, which must be completely removed before the modRNA is packaged into the lipid nanoparticles (“LNPs”). It has since been found that the RNA-based injections are contaminated with significant amounts of DNA (plasmid DNA).
There are various conceivable mechanisms, including plasmid DNA impurities, for the triggering of serious adverse effects.
The best documented adverse effects are inflammations caused by the body’s own immune system reacting against the foreign spike protein produced in the body’s cells. Particularly prominent are inflammations of blood vessels, heart muscle, lungs, skin, liver, kidneys and nervous system.
There are also indications that RNA-based injections weaken the immune system’s defence function. This is reflected in the increased number of cases of shingles and bacterial infections such as appendicitis, and wound and prosthesis infections.
Additionally, an increased number of fast-growing tumours, including malignant lymphomas and leukaemias, have been observed in vaccinated people. The exact mechanism of triggering these malignant diseases is not yet fully understood but both the spike protein and the nucleic acid precursors (modRNA and DNA) could play a role. The aforementioned immunosuppression is probably also involved.
For further information on covid vaccine harms, please refer to the book ‘mRNA Vaccines Toxicity’ published by Doctors for Covid Ethics (“D4CE”).
It is possible to detect certain components in covid “vaccines” even months after the injection using special tests of blood, cerebrospinal fluid or tissue samples (biopsy), which can be used as evidence of vaccine damage in an expert opinion.
“The documentation and, if necessary, publication of vaccine damage is particularly important because, among other things, it can be used to gather arguments against the further continuation and authorisation of the gene-based vaccine, which has not yet been fully tested, and thus possibly save other people similar suffering,” Inmodia says.
Inmodia offers three tests specifically for injection-derived components: detection of spike protein (Wuhan type), detection of spike-modRNA and detection of plasmid DNA. However, specific detection methods for DNA-based injections are currently not offered, as they have hardly been used in Germany and only general spike protein detection is possible for the time being.
Inmodia recommends that people who would like to have tests done start with the detection of spike protein, which requires, if possible, the testing of tissue samples (biopsies), alternatively or additionally blood samples can be tested. This is because the detection of nucleic acids (modRNA and DNA) is significantly more time-consuming and cost-intensive and it should generally only be considered after positive detection of spike protein.
You can view a full list of possible tests and prices HERE. [archive]
Italian Soccer Match Suspended After 22-Year-Old Player Collapses Suddenly on Pitch (VIDEO)
Ed.:
Man Regains Consciousness Moments Before Cremation; Three Government Hospital Doctors Suspended
[Ed.: Quack-quack! Would it be premature to declare medicine dead?]

Americans Who Have Never Been “Vaccinated” for ANYTHING Are the Healthiest Among Us 2ND SMARTEST GUY IN THE WORLD
DEC 01, 2024
This Substack has long been exposing the deadly and highly profitable medical fraud known as vaccines. There is not a single high quality, well designed, large sample size random controlled trial (RCT) with placebo control group for any vaccine.
The following breakdown of the childhood vaccine schedule — even the pair of placebo group trials that are of incredibly low quality, demonstrate how especially unsafe those respective products are precisely because that pair of trials were more robust, thus better establishing how dangerous and unnecessary they really are — proves that not a single one of these vaccines would ever be approved in an honest regulatory process:
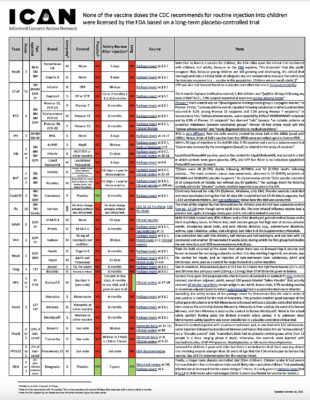
But what we do finally have is an exceptionally high quality and highly robust RCT entitled, Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders, which concluded:
Forensic Pathologist: Covid ‘Vaccines’ Behind Spike in Violent Sudden Seizure Deaths By Frank Bergman
One of America’s leading forensic pathologists has issued a red alert after proving that Covid mRNA “vaccines” are behind recent spikes in violent sudden seizure deaths.
November 29, 2024 – One of America’s leading forensic pathologists has issued a red alert after proving that Covid mRNA “vaccines” are behind recent spikes in violent sudden seizure deaths.
An investigation into the fatal seizures was led by forensic pathologist Dr. Joseph A. Prahlow.
Prahlow is a Professor of Pathology at St. Louis University School of Medicine and the Assistant Medical Examiner at the City of St. Louis’s Office of the Medical Examiner.
The renowned expert is now raising the alarm after discovering that once-rare seizures are a terrifying adverse effect of Covid mRNA injection.
Prahlow revealed that he investigated cases where no alternative cause could be identified, proving, without doubt, that the “vaccines” caused the fatal seizure spike.
The findings were published in the peer-reviewed journal Academic Forensic Pathology.
Prahlow’s paper presents two cases of new-onset seizures resulting in death shortly after vaccination as supporting evidence.
However, Prahlow warns that many other cases of sudden fatal seizures haven’t been investigated, meaning global spikes in such deaths are also likely linked to the mass Covid vaccination campaign.
The cases presented in the paper raise important questions about causality, clinical management, and death certification.
This thorough case analysis involves the meticulous examination of two cases, detailing the clinical history, diagnostic work-ups, and forensic findings.
The methodical approach used during the investigation ensures that potential contributing factors are explored comprehensively.
However, similar deaths are not normally investigated so thoroughly so the actual causes are not usually identified.
During his investigations, Prahlow identified a direct connection between Covid mRNA vaccination and sudden seizure mortality.
When determining the plausibility of vaccine-induced seizures, Prahlow’s paper highlights the established frameworks, such as the World Health Organization’s (WHO) causality assessment criteria and Brighton Collaborative Criteria.
The paper also identifies other neurological adverse events associated with “vaccines,” such as encephalitis and stroke.
These broader neurological effects could provide additional insights into the mechanisms of vaccine-induced seizures.
This study contributes meaningfully to the discussion on vaccine safety by shedding light on rarely-discussed adverse events like seizure-related deaths.
While it highlights areas for improvement in clinical and forensic practice, it also emphasizes the need for balanced, evidence-based approaches that prioritize both individual and public health considerations.
Further research and stronger surveillance systems are essential to better understand and mitigate such risks.
Dr. Prahlow effectively links vaccination to mortality, emphasizing the importance of considering vaccines as potential contributors when no other explanation is evident.
This highlights the need for diligence in vaccine-related adverse event investigations.
The paper concludes by stressing the importance of informed consent, especially given the “fast-tracked” nature of COVID-19 vaccines.
Patients must be made aware of all potential risks, even rare ones, to make truly informed decisions.
This is not the first study to link Covid mRNA “vaccines” to deadly seizures, however.
As Slay News previously reported, a peer-reviewed study published in the prestigious Cureus Journal earlier this year analyzed the death of a man who was killed by seizures within 40 hours of receiving a Covid mRNA injection.
The researchers documented the case of the 73-year-old man who had received a Pfizer mRNA Covid shot.
He developed a headache that was followed by violent seizures, loss of consciousness, and finally death.
The case is a cause for concern as the man was killed in under two days after being injected, the researchers note.
The study, conducted by world-renowned Japanese scientists Shimura M, Fujikawa H, Yazawa M, et al., is titled “An Autopsy Case of Reversible Cerebral Vasoconstriction Syndrome After a Severe Acute Respiratory Syndrome Coronavirus 2 Vaccination.”
The scientific study determined that a form of brain damage can occur rapidly after a person is injected with a Covid mRNA shot.
Meanwhile, the U.S. Food and Drug Administration (FDA) revealed last year that a safety signal has been detected that suggests Covid mRNA shots may be linked to a spike in seizures among toddlers following vaccination.
As Slay News reported, researchers with the FDA and three large healthcare companies revealed the findings in a new preprint study.
The study shows that seizures/convulsions “met the statistical threshold for a signal” in children aged 2 to 4 following receipt of a Pfizer COVID-19 vaccine.
The same safety signal was also detected among children aged 2 to 5 following receipt of a Moderna COVID-19 vaccine.
Source: slaynews.com
[Ed.: The pun ‘spike’ in the title does not go unnoticed!]
COVID-19 (& Parkinson’s) Cured, Advanced Cancer Full Remission & Breast Cancer Patient “Cancer Free” After Ignoring Radiation Oncologist Advice to STOP Ivermectin 2ND SMARTEST GUY IN THE WORLD
This article is too long for email and should be opened in a browser.
NOV 30, 2024 – We have yet another trio of inspirational success stories using inexpensive repurposed drugs that the Medical Industrial Complex does not want anyone to know about.
Our first subscriber success story comment is especially intriguing because we know that Ivermectin instantly cures COVID-19, or why the criminals went after it so hard to ensure that they could obtain their fraudulent FDA Emergency Use Authorization for their slow kill bioweapon “vaccines;’ but once again this Nobel Prize winning miracle drug has some very important “side effects:”
Readers of this Substack appreciate that Ivermectin is effective for not just prion-based diseases like Alzheimer’s and dementia, or VAIDS-induced early onset versions of these conditions, but that it could also address a wide range of neurodegenerative diseases like Parkinson’s that “experts” claim there are no cures for; to wit:
JUL 11
The next two success stories share a similar theme in that the “expert” doctors insult and devalue their patients in order to better control them.
A few weeks ago the following email landed in my inbox:
[Ed.:
