
COVID-19 / Malicious Medical Quackery
[Ed.: FEAR YOUR DOCTOR! Medicine is a disgraced profession. They cannot (and must not) be trusted any longer! Cultivate Nosocomephobia and iatrophobia. Spread ‘vaccine hesitancy’! How Bad is My Batch?
If you know someone injured by the jabs, direct them to humanitysuit.com to become a plaintiff.]
How Bad is My Batch? Enter your batch number(s) and find out. Then take action and purge yourself of this shit to the extent possible. It’s do-able!]
MUST-WATCH: Dr. Yeadon Explains Why the So-called Covid-19 Vaccines Were “DELIBERATELY DESIGNED… To Injure, Kill and Reduce Fertility.” [15:32] LIONESS OF JUDAH MINISTRY MAR 21, 2025
“The people designing these… knew these things were going to happen, and that’s why I say it’s intentional.”
Dr. Mike Yeadon, former vice president and chief scientific officer at Pfizer, explains why the so-called Covid-19 vaccines were “deliberately designed… to injure, kill and reduce fertility.”
“This is an allegation I’ve been making for around three and a half years… If I was wrong, I would have expected the drug companies whose products I am maligning to have… secured a court injunction to stop me repeating these allegations.”
“The people designing these… knew these things were going to happen, and that’s why I say it’s intentional.”
“I wish I didn’t have to communicate this information, but there is no possibility that the people involved in designing these products did not know that they would have the effects that I predicted, and that so many people have actually experienced.”
Full Video [15:32]
Spike – Part 2. mRNA injection-induced fibrous clots may be crosslinked fibrin. SASHA LATYPOVA
Brainwashed scientists from UCSF published a paper accidentally explaining the white fibrous clots found by morticians in mRNA vaccine victims worldwide.
OCT 17, 2024 – First a note of gratitude for the notes from paid subs. I can’t answer each and every one, so I am going to say it here – thank YOU! I am reading your notes and I very much appreciate your support. Writing this substack is a full time job. Art is an after hours job. And I love it, or I wouldn’t be doing it. Your messages are inspiring and telling me I should continue, and I will.
A recent paper from UCSF published in Nature, despite efforts of the authors to cover up mRNA vaccine injury, revealed some very interesting findings. It may potentially explain those huge rubbery clots that are being pulled from the deceased vaccine victims by morticians, and on occasion have been extracted from people who are still alive.
Here is an excellent article discussing “People’s Blood Clot Survey” with harrowing statistics about these clots:
Clotastrophe
Results of the People’s Blood Clot Survey as of October 1, 2024
Read more https://laurakasner.substack.com/p/results-of-the-peoples-blood-clot
5 months ago · 53 likes · 35 comments · Laura Kasner
These clots are not assembled from the contents of the vials, but only “ignited” by them as will be explained below. There is not enough volume of the injectable to account for such large structures, so these clots contain accumulated human tissue for the most part.
Major findings from the USCF study:
- Fibrin and fibrinogen bind to the spike protein and form proinflammatory blood clots.
- Clots drive systemic thrombo-inflammation, micro- and macro-clotting & brain pathology.
- Loss of natural killer (NK) cells is seen & explains increase in cancer.
Some basic facts about fibrin and fibrinogen:
Fibrin and fibrinogen are two closely related proteins that play a crucial role in blood coagulation and hemostasis. Fibrinogen is synthesized in the liver, in hepatocytes. Fibrinogen is present in normal blood in high concentrations but lies dormant until activated, typically in response to a vascular injury. The subsequent cascade produces fibrin. Fibrin is required when there is injury to blood vessel walls, a foreign substance in the body (e.g., an injected toxic mRNA concoction) and/or through activated cells.
Formation of fibrin clots in vivo, their size, and location, as well as fine structure and properties are greatly influenced by several variable pathogenic factors shown in the upper part of the cartoon below. The biological and clinical relevance of fibrin is determined by its implications in the vital interconnected patho (physiological) reactions and processes:

In the process of fibrin formation, fibrinogen is cleaved into fibrin monomers (single strands) which assemble into a tough insoluble matrix of fibers that coagulates blood which forms a clot. This is normally a reversible reaction. The body can dissolve fibrin clots through a series of enzymatic reactions after the wound has healed and the clot is no longer needed.
More recently, fibrin has been used as a versatile biomaterial, particularly in surgical applications as a sealant, gel, cellular matrix, scaffolding, etc. This is because some permanent structures can be made out of it, as long as the dissolution of fibrin is prevented by the prosses of cross-linking.
This scientific review paper about fibrin states that:
Fibrin formation is naturally reversible but the fibrin network can be made permanent through crosslinking with various other polymers [14]. The fibrin clot that is crosslinked yields a stronger clot mechanically, with higher stability and resistance to breakdown by the body. Fibrin clots also generally attract and bind to various plasma proteins in the body. Some examples include actin, cadherin, albumin and interleukin-1β among others.
In chemistry and biology, a crosslinking is formation of bonds or a short sequences of bonds that links one polymer chain to another. When polymer chains are crosslinked, the material becomes more rigid.
Would spike protein count among these “plasma proteins” that bind and crosslink with fibrin, forming a permanent, non-dissolvable fibrous clot? Methinks it’s highly likely!
Lo and behold, that’s exactly what the UCSF study published in Nature found. Fibrin-fibrinogen-spike interaction in clot formation:
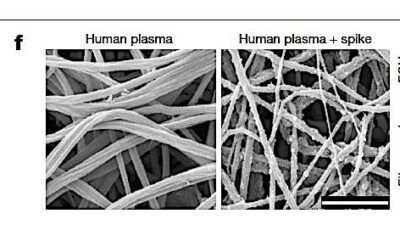
The picture is worth a 1000 words. You can see the spikes bound into fibrin, creating sticky points, and crosslinks, leading to permanent fibrous structures, that can no longer be dissolved by the body. I added emphasis and annotations in the below quote from the UCSF study:
We next tested whether spike interferes with the polymerization, degradation and inflammatory properties of fibrin. Incubation of spike with healthy donor plasma in the presence of thrombin, which is elevated during COVID-19 [read – mRNA injection], resulted in altered clot structure shown by scanning electron microscopy (SEM) and increased turbidity of fibrin clot formation (Fig. 1f,g and Extended Data Fig. 3a–c). Incubation of spike with fibrin delayed plasmin degradation of both the β-chain and the γ–γ dimer (Fig. 1h), suggesting that spike delays fibrinolysis. These findings are consistent with the formation of dense fibrin clots with thin fibres in thromboembolic diseases and fibrinolysis-resistant blood clots in patients with COVID-19 [read – in mRNA vaccine victims].
So, these guys from UCSF found that the spike (ONLY FROM “DA VIRUS”, I SWEAR!!) activates fibrin formation, then binds and polymerizes the fibrin into permanent, non-dissolvable structures. Lovely. This might explain those embalmer clots, seems like a plausible mechanism to me.
What if this happens in the brain? Or, even better – in the testicles of the vaxxed clowns from UCSF who wrote this paper (I am sure they gulped a few times when looking at their own results). Not good. Not good at all:
Increased BBB permeability associated with parenchymal fibrin deposition is a feature of COVID-19 neuropathology8,9. In the brain of some patients with COVID-19, detection of spike and viral RNA suggests potential neuroinvasion41,45.
By now you all know to replace “covid-19” with “mRNA injections” while reading propaganda journals like Nature, right?
Our data and previous literature support that, while spike can enhance fibrin toxicity, even in the absence of spike, fibrin is deleterious in diseases such as multiple sclerosis, Alzheimer’s disease, rheumatoid arthritis, colitis and periodonditis15,18,19,20. Thus, fibrin may be deposited either together with spike when spike is present in the brain45 or through an open BBB after peripheral infection without neuroinvasion or spike coupling.
Among other goodies from injecting mRNA and/or spike in LNP they also found that fibrin suppresses “natural killer” (NK) cells that are supposed to keep cancer in check. So, are we shocked that mRNA-induced turbo cancer is out of control?
The fibrin-induced suppression of NK cells that we observed is consistent with enhanced cancer cell survival in vitro after co-culture with fibrin-stimulated NK cells48, suggesting a role for fibrin in other diseases with vascular damage and impaired NK cell cytotoxicity, such as cancer and autoimmune diseases49.
Conclusion from UCSF study:
These results suggest a fibrin-dependent mechanism that elicits inflammatory and oxidative stress responses in the presence of spike in the absence of active infection, which could therefore have a role in long COVID.
In other words, the authors conclude that spike protein, circulating in the blood in the absence of “active covid infection” is responsible for clotting and fibrin crosslinking. What is the spike doing in the blood when there is no “infection”? It’s like saying, there was a shark in these waters 2 years ago, he left and we haven’t seen him again, but the teeth, man! They swim and multiply now all by themselves… We must call it the Long Shark Syndrome, otherwise Nature will ban us… Let’s think hard about this… Think harder…. Oh! I know! It’s when the spike and numerous vectors for it are injected into the blood stream by a needle, isn’t it, that’s when we arrive at this highly unfortunate situation.
But of course, the acadummies from UCSF must never think such unauthorized thoughts. They immediately plead that this clearly vaccine-induced scenario is not vaccine induced:
Notably, we do not believe that this mechanism is related to the rare clotting complications observed with adenovirus based COVID vaccines because the production of anti-PF4 autoantibodies and ensuing drop in platelet counts are triggered by the vector rather than spike36.
Well… maybe just a little bit true. “Small amount”… “accumulate locally” and then swiftly eliminated… and unlike those BAD spikes, these are GOOD spikes, see, the BAD ones make crosslinked fibrin clots, but the GOOD ones make you go to heaven:
In general, COVID-19 RNA vaccines lead to small amounts of spike protein accumulating locally and within draining lymph nodes where the immune response is initiated and the protein is eliminated37. Consistent with the safety of the spike mRNA vaccines, mRNA vaccines prevent post-COVID-19 thromboembolic complications38 and a cohort study in 99 million COVID-vaccinated individuals showed no safety signals for haematological conditions39.
It’s hard to be an acadummy-scientist these days: you have to twist into illogical pretzels, but anyone with a non-smooth brain can see you are just a pathetic small-money whore.
Titanium Dioxide Nanoparticles Don’t Belong in our Food Supply NICOLAS HULSCHER, MPH
HHS-led food supply clean up operations are more important than you may think.
MAR 20, 2025 – On Fox News this morning, RFK Jr. reaffirmed that:
We told them that we wanted the dyes out of the foods. The science on the dyes is so overwhelming … We’re going to get rid of the GRAS (Generally Recognized As Safe) standards for most products … That designation was expanded … so that any new chemical they want to add to our food is generally recognized as safe and gets no review. That’s why we have 10,000 ingredients in our food in this country. In Europe, they only have 400, and we have the worst chronic disease burden of any country in the world.
Having public health agencies that actually care about the safety of our food supply is huge news, and I’ll give a concrete example as to why.
In the United States, titanium dioxide (TiO₂) nanoparticles, often labelled as E171, are used as a color additive in over 3,000 different food products. Primarily used in candy, titanium dioxide is also present in salad dressings, chewing gum, ice cream, frozen pizzas, drink and gelatin mixes, and various other food products. It enhances color by providing a smooth finish while increasing shine and brightness. Despite it’s appearance-altering properties, titanium dioxide as a food additive is banned in Europe due to safety concerns.
The study titled, Ingestion of titanium dioxide nanoparticles: a definite health risk for consumers and their progeny, revealed the systemic heath risks of this synthetic additive:
Titanium dioxide (TiO2) is one of the most commonly used nanomaterials in the world. Additive E171, which is used in the food industry, contains a nanometric particle fraction of TiO2. Oral exposure of humans to these nanoparticles (NPs) is intensive, leading to the question of their impact on health. Daily oral intake by rats of amounts of E171 that are relevant to human intake has been associated with an increased risk of chronic intestinal inflammation and carcinogenesis. Due to their food preferences, children are very exposed to this NP. Furthermore, maternal-foetal transfer of TiO2 NPs during pregnancy, as well as exposure of the offspring by breastfeeding, have been recently described. In France, the use of E171 in the production of foodstuffs was suspended in January 2020 as a precautionary measure. To provide some answers to this public health problem and help global regulatory agencies finalize their decisions, we reviewed in vitro and in vivo studies that address the effects of TiO2 NPs through oral exposure, especially their effects on the gastrointestinal tract, one of the most exposed tissues. Our review also highlights the effects of exposure on the offspring during pregnancy and by breastfeeding.
This is what titanium dioxide nanoparticles do to intestinal microvilli:
Largest Ever Covid ‘Vaccine’ Study Confirms 610% Spike in Heart Failure Frank Bergman
March 20, 2025 – The largest study ever conducted for Covid mRNA “vaccines” has confirmed that the injections have caused an alarming surge in heart failure and other deadly adverse events.
A team of 22 leading researchers at the Global Vaccine Data Network (GVDN) analyzed the records of a whopping 99,068,901 “vaccinated” people for the peer-reviewed study.
The study’s paper was published in the prestigious journal Vaccine.
In total, the study investigated 183,559,462 doses of mainly Pfizer, Moderna, and AstraZeneca.
The researchers found that most of the severe side effects occurred within 43 days of receiving the injection.
There were unacceptable population risks of Guillain-Barré syndrome, blood clots, encephalomyelitis, heart failure (myopericarditis and pericarditis), and swelling in the brain and spinal cord.
The study identified massive spikes in serious health conditions among individuals who had received Covid shots.
Leading epidemiologist Nicolas Hulscher MPH responded to the study by warning that Covid mRNA injections are “NOT SAFE FOR HUMAN USE”
In a post on X, Hulscher noted that the study confirms:
➊ 610% increased risk of myocarditis following mRNA platform injection.
➋ 378% increased risk of acute disseminated encephalomyelitis (ADEM) following mRNA injection.
➌ 323% increased risk of cerebral venous sinus thrombosis (CVST) following viral-vector injection.
➍ 249% increased risk of Guillain-Barré syndrome (GBS) following viral-vector injection.
The study concludes by warning that “Other potential safety signals that require further investigation were identified.”
Meanwhile, another major autopsy study has found that people who died from a sudden cardiac arrest had multiple scars in their hearts caused by Covid mRNA “vaccines.”
The study was conducted by cardiologist Dr. Tomomi Koizumi and pathologist Dr. Masao Ono of the Mito Medical Center in Higashi-Ibarakigun, Japan.
NEW AUTOPSY STUDY – Cardiac Micro-Scars in Sudden Death Following COVID-19 Vaccination NICOLAS HULSCHER, MPH
Corroborates our prior research on COVID-19 vaccine-induced cardiac arrest, reinforcing the link between myocardial scarring, arrhythmias, and sudden death.
MAR 19, 2025
The study titled, Cardiac Multiple Micro-Scars: An Autopsy Study, was just published in JACC: Case Reports:
Background
Unexplained cardiac arrest is often attributed to a patient’s underlying disease. However, it is well known that an autopsy can reveal pathologies that were not noticed before death.
Case Summary
Multiple micro-scars (MMS) found in the myocardium of 3 patients who died of unexplained cardiac arrest were presented at our clinicopathology conference. Upon review of the clinical record, patients with MMS before death had arrhythmia (ie, atrial fibrillation and nonsustained ventricular tachycardia, including new onset). Interestingly, MMS were found in the left ventricle, the junction of the pulmonary vein and left atrium, and the right ventricle and right atrium. All 3 patients had histories of COVID-19 booster vaccination, and 1 of the 3 patients had a history of COVID-19.
Discussion
For patients with unexplained cardiac arrest complicated with arrhythmia, cardiac MMS is given as the differential background disease.
All three patients had received multiple COVID-19 booster injections (Patient 1: 5 doses, Patient 2: 5 doses, Patient 3: 6 doses). One patient had a confirmed history of COVID-19 infection.
The Authors speculate a connection between COVID-19 vaccination and cardiac scarring due to:
- Spike protein production, triggering immune activation, inflammation, microvascular injury, and fibrosis—leading to myocardial scarring and electrical instability.
- Microvascular injury and thrombotic microangiopathy, causing localized ischemia and scarring.
Patients exhibited arrhythmias before death, including atrial fibrillation and nonsustained ventricular tachycardia. Micro-scars were notably found in regions associated with atrial fibrillation origins, such as the pulmonary vein-left atrium junction. The scars appeared evenly spaced in the myocardium, suggesting a systemic inflammatory or microvascular process:
This study provides further insight into the syndrome known as COVID-19 vaccine-induced cardiac arrest, which we previously elucidated in our recently published paper, Risk Stratification for Future Cardiac Arrest After COVID-19 Vaccination. Our prior research identified subclinical myopericarditis and small patches of myocardial inflammation or fibrosis as potential triggers for reentrant ventricular tachycardia, ultimately leading to sudden cardiac arrest. Notably, our work also highlighted the presence of vaccine-derived Spike protein in myocardial tissue, implicating it as a driver of persistent cardiac inflammation and injury.
The detection of multiple micro-scars (MMS) in this study aligns with our proposed mechanism, where Spike protein-induced microvascular injury and inflammatory responses may lead to myocardial scarring, electrical instability, and lethal arrhythmias. Given that small myocardial lesions can be missed on routine imaging or autopsy, our findings further reinforce the necessity for systematic risk stratification—including biomarker assessment for circulating Spike protein, cardiac imaging, and histopathological analyses—to identify individuals at heightened risk of post-vaccination cardiac events.
Unfortunately, no testing for Spike protein or vaccine mRNA was conducted in the MMS study. Such testing should be a standard part of autopsy investigations following COVID-19 vaccination, as outlined in our study Delayed Fatal Pulmonary Hemorrhage Following Covid-19 Vaccination: Case Report, Batch Analysis, And Proposed Autopsy Checklist:
As indicated by our study, A Systematic Review of Autopsy Findings in Deaths After COVID-19 Vaccination, the cardiovascular system is the most frequently implicated in COVID-19 vaccine-induced deaths. Notably, sudden cardiac death was identified as the cause of death in 35% of positively adjudicated cases:
COVID-19 vaccine-induced cardiac arrests are expected, given that the vast majority of the population received at least one dose of a cardiotoxic mRNA injection. Our study, Excess Cardiopulmonary Arrest and Mortality after COVID-19 Vaccination in King County, Washington, found a 1,236% surge in excess cardiac arrest deaths following the mass vaccination campaign among a sample size of 2 million COVID-19 vaccinated individuals:
Epidemiologist and Foundation Administrator, McCullough Foundation
www.mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
BREAKING STUDY: The Disastrous COVID-19 Response Led to Mass Harm and Death NICOLAS HULSCHER, MPH
How government censorship, corruption, and the suppression of life-saving treatments fueled unnecessary suffering, silenced doctors, and cost countless lives.
MAR 19, 2025
The study titled, A Narrative Review of the COVID-19 Infodemic and Censorship in Healthcare, was just published in the journal Secrecy and Society:
Abstract
Ideological and financial motivations have undermined science for decades. In this narrative review, we explore how organizations and governments used misinformation, disinformation, censorship, and secrecy to manage the COVID-19 pandemic. Various rationales for employing censorship and secrecy during the COVID-19 pandemic are examined including how organizations and governments create confusion about the risks associated with their products and blame avoidance to shift responsibility and to avoid accountability for their actions. Methods of censorship employed during the COVID-19 pandemic are reviewed, examples are provided, and the consequences of these actions are reviewed. Information included in this review was obtained from scientific papers, government documents, mass media articles, books, and personal accounts of physicians and scientists. We examine how the use of censorship and secrecy created a challenge for scientists, physicians, politicians, and the general public in trying to understand COVID-related topics. Finally, strategies for managing censorship and secrecy during a pandemic are presented.
Here are the key highlights of the study:
1. COVID-19 Response Was Driven by Secrecy, Censorship, and Misinformation
- Governments and global health organizations deliberately manipulated information to control public perception.
- The response was not guided by science but by political and financial interests.
- Censorship of dissenting voices was rampant, with doctors, scientists, and journalists punished for questioning the official narrative.
2. Suppression of Scientific Debate on the Origins of SARS-CoV-2
- Early in the pandemic, any discussion of a possible lab-leak origin was dismissed as a “conspiracy theory”—despite evidence linking SARS-CoV-2 to gain-of-function research funded by the U.S. government.
- Government agencies and social media platforms actively silenced discussions and suppressed independent investigations.
- Whistleblowers revealed efforts to manipulate scientific conclusions—including CIA interference to shift findings in favor of a natural origin.
3. COVID-19 Vaccines Were Overhyped, Unsafe, and Mandated Through Coercion
- The claim that vaccines prevented transmission was false, yet mandates were aggressively enforced.
- Evidence of serious adverse effects was ignored or actively covered up by regulatory agencies.
- Doctors who raised concerns about vaccine safety or efficacy were censored, lost their medical licenses, and faced legal threats.
- The media and Big Tech worked with governments to smear critics, branding them as “anti-science” or “dangerous.”
4. Cheap, Effective COVID-19 Treatments Were Suppressed to Protect Vaccine Profits
- Repurposed drugs like ivermectin (IVM) and hydroxychloroquine (HCQ) were demonized—despite strong evidence they worked.
- Physicians were blocked from prescribing these treatments, and pharmacists were instructed not to fill prescriptions.
- The FDA and CDC colluded with Big Pharma to push expensive, patented drugs like Remdesivir and Paxlovid instead.
5. Lockdowns, Social Distancing, and Mask Mandates Were Not Backed by Science
- Lockdowns caused immense harm, especially to children and small businesses, but were implemented based on fear, not data.
- The “6-foot rule” was a baseless guideline—even Dr. Fauci later admitted it “just appeared” without evidence.
- Governments and media silenced opposition, including world-renowned epidemiologists behind the Great Barrington Declaration, which advocated for a focused protection approach instead of mass lockdowns.
6. Media and Tech Companies Served as Enforcers of Government Censorship
- Big Tech platforms like Facebook, Twitter, and YouTube colluded with government agencies to censor dissenting voices.
- Scientific journals retracted papers that challenged the COVID-19 narrative, regardless of the quality of research.
- People lost their jobs, bank accounts were frozen, and financial institutions “debanked” individuals for speaking out against mandates and restrictions.
7. The COVID-19 Response Was the Most Widespread Attack on Free Speech in Modern History
- Government agencies weaponized the term “misinformation” to silence legitimate scientific debate.
- Doctors, scientists, and politicians were blacklisted for questioning the vaccines or advocating for alternative treatments.
- Legal battles are now exposing how the government colluded with private companies to suppress free speech and manipulate public opinion.
Clearly, the COVID-19 response was a disaster driven by corporate greed, political control, and a suppression of medical autonomy. Restoring scientific integrity requires full transparency, accountability, and consequences for those who orchestrated the censorship and coercion. Future public health emergencies must not be left in the hands of corrupt institutions that prioritize profits and power over human lives.
Nicolas Hulscher, MPH Epidemiologist and Foundation Administrator, McCullough Foundation
www.mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
Japan Issues Alert as Vaccinated Child Deaths Surge Frank Bergman
March 18, 2025 Slay News – Leading experts in Japan have issued a global alert to call for an urgent reassessment of worldwide vaccination programs after linking a recent surge in child deaths to “vaccines.”
A bombshell new study published in the Springer Nature peer-reviewed journal Discover Medicine raises the alarm over the issue after connecting several child deaths to “vaccinations.”
However, it wasn’t only mRNA injections that were linked to the deaths as the study found that multiple children died suddenly after receiving standard childhood schedule vaccines.
The study was conducted by Dr. Kenji Yamamoto of Okamura Memorial Hospital in Japan.
In the wake of Yamamoto’s, top Japanese experts are now calling for an urgent reassessment of global vaccination programs, particularly mRNA “vaccines.”
Yamamoto’s findings are driven by growing evidence of vaccine-induced immunodeficiency and a sharp rise in adverse effects.
Alarmingly, Japan has recorded over 600,000 excess deaths since the Covid “vaccine” rollout.
However, despite the pandemic long being over and “vaccine” uptake waning, deaths have continued.
Particularly concerning are the soaring deaths among children who received Covid injections.
During the study, Yamamoto analyzed dozens of unexplained child deaths in Japan.
He found that sudden and mysterious child deaths skyrocketed after Japanese kids were given Covid vaccines.
However, Yamamoto noted that three unexplained child deaths investigated for the study occurred within a day of a routine vaccination.
Dr. Yamamoto warns that these shocking statistics warrant further investigation.
Despite detailed autopsy reports, experts classified these cases as “causality unassessable.”
This classification prompted Yamamoto to question whether external pressures or conflicts of interest may be obstructing proper vaccine safety evaluations.
This is a serious matter that needs to be taken seriously in the United States.
Experts are now urging pro-safety Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. to examine Dr. Yamamoto’s findings.
The study traces how most countries worldwide have halted additional mRNA doses.
However, places like Japan and America are the exception and continue administering eighth-dose boosters to the elderly.
This comes despite concerns over immune system depletion, IgG4 antibody surges, and rising infection rates post-vaccination.
What is unique about Yamamoto’s study is his investigations target other vaccines as well.
In the study’s paper, Yamamoto the three deaths among children who received non-Covid “vaccines.”
The youngest was a two-month-old baby boy who died one day after receiving HIB, rotavirus, and pneumococcal shots.
The infant, who died on January 23, 2024, suddenly fell ill 30 minutes after the injections.
He went into asystole in the hospital 59 minutes after being vaccinated.
In another case, a six-month-old baby girl died within one day of receiving shots for hepatitis B, HIB, pneumococcal, and a four-in-one vaccine (pertussis, diphtheria, tetanus, polio).
She was found dead on November 24, 2023 – the day after the “vaccines.”
The third case was a three-year-old boy who died one day after receiving the Japanese encephalitis vaccine.
He appeared lethargic and had a fever of 103 °F approximately 8 hours after the vaccine and he died shortly after.
Yamamoto highlights fundamental flaws in vaccine monitoring and classification.
He points out that most deaths occurring immediately after vaccination are systematically labeled as “unable to assess” rather than being rigorously examined.
The doctor argues that vaccination policies have been shielded from scientific scrutiny.
Regulators and industry insiders are dismissing mounting concerns while failing to validate long-term safety.
The study proposes pre-vaccination blood tests to detect potential immune vulnerabilities before administering shots and urges an immediate reassessment of regulatory bodies, including replacing officials with conflicts of interest.
Yamamoto stops short of calling for a total vaccine moratorium.
However, he strongly recommends suspending current programs until comprehensive, double-blind, long-term clinical trials can validate safety.
These bold assertions are supported by troubling real-world data and pose a challenge to public health authorities, vaccine manufacturers, and media narratives that continue to frame questioning vaccination as “anti-science.”
Yet, the publishing of Yamamoto’s study in the Springer Nature Discovery Medicine signals a new openness for mainstream publishers to start exposing the problem.
The study, which received no external funding, is a stark reminder that scientific inquiry must remain untainted by political and financial pressures, especially when human lives are at stake.
READ MORE – FDA Admits Covid mRNA ‘Vaccines’ Cause Cancer
MAHA Must Correct Vitamin D RDAs—Public Health Depends on It NICOLAS HULSCHER, MPH
A statistical error in the recommended dietary allowance (RDA) for vitamin D has led to inaccurate guidelines with serious public health consequences.
MAR 18, 2025
A study titled, The Big Vitamin D Mistake, published in the Journal of Preventive Medicine & Public Health, reported the following:
Since 2006, type 1 diabetes in Finland has plateaued and then decreased after the authorities’ decision to fortify dietary milk products with cholecalciferol. The role of vitamin D in innate and adaptive immunity is critical. A statistical error in the estimation of the recommended dietary allowance (RDA) for vitamin D was recently discovered; in a correct analysis of the data used by the Institute of Medicine, it was found that 8895 IU/d was needed for 97.5% of individuals to achieve values ≥50 nmol/L. Another study confirmed that 6201 IU/d was needed to achieve 75 nmol/L and 9122 IU/d was needed to reach 100 nmol/L. The largest meta-analysis ever conducted of studies published between 1966 and 2013 showed that 25-hydroxyvitamin D levels <75 nmol/L may be too low for safety and associated with higher all-cause mortality, demolishing the previously presumed U-shape curve of mortality associated with vitamin D levels. Since all-disease mortality is reduced to 1.0 with serum vitamin D levels ≥100 nmol/L, we call public health authorities to consider designating as the RDA at least three-fourths of the levels proposed by the Endocrine Society Expert Committee as safe upper tolerable daily intake doses. This could lead to a recommendation of 1000 IU for children <1 year on enriched formula and 1500 IU for breastfed children older than 6 months, 3000 IU for children >1 year of age, and around 8000 IU for young adults and thereafter. Actions are urgently needed to protect the global population from vitamin D deficiency.
Let’s expand on some the main points:
Statistical Error in Vitamin D RDA
The statistical error in the estimation of the Recommended Dietary Allowance (RDA) for vitamin D occurred because the Institute of Medicine (IOM) misinterpreted its own statistical analysis. The IOM estimated that 600 IU/day of vitamin D would ensure that 97.5% of individuals reach a serum 25-hydroxyvitamin D (25(OH)D) level of 50 nmol/L. However, their calculation was incorrect because they mistook the lower prediction limit for individuals as the lower limit for group averages. A reanalysis by Veugelers and Ekwaru showed that 600 IU/day only ensures that 97.5% of study averages (not individuals) exceed 50 nmol/L, while actual individual requirements vary significantly. Their corrected calculation found that 8895 IU/day was needed to ensure that 97.5% of individuals reach the target level, a number vastly higher than the IOM’s recommendation :
5G? – The Cancer Shadow of RF Radiation: A Threat Buried by Profit Tom Renz
MAR 18, 2025 – We’re constantly blasted by radiofrequency (RF) radiation—cell phones glued to our ears, WiFi routers in every home, and 5G towers blanketing our skylines – especially in urban areas. It’s a trillion-dollar industry, raking in cash for telecom giants while the government sets exposure limits that whisper a chilling truth: RF isn’t harmless. The Occupational Safety and Health Administration (OSHA) caps RF at 10 mW/cm² for workers (29 CFR 1910.97)[1], and the Federal Communications Commission (FCC) restricts public exposure to 1.6 W/kg localized SAR and 0.08 W/kg whole-body (47 CFR 1.1310)[2]. These aren’t decorative rules—they’re admissions that RF can hurt us, built to stop heat from frying tissue. But cancer doesn’t need a burn to take root; it can form from other mechanisms such as a cascade of reactive oxygen species (ROS) or cell membrane disruption. I’m not a doctor but I’ve been looking at the evidence and this appears to be another case where our federal government will not fund studies because they – or more accurately those that buy off our federal officials – do not want the truth.
Regulatory Limits: A Warning, Not a Shield
The rules themselves peel back the curtain on RF’s danger. OSHA’s 10 mW/cm² threshold, etched into law for telecom workers near antennas (29 CFR 1910.97)[1], isn’t there to coddle—it’s a bulwark against RF’s ability to cook flesh, spark burns, or drive heat stress. The FCC sharpens this further, pegging your phone at 1.6 W/kg SAR and ambient exposure at 0.08 W/kg, with power density tuned to 1 mW/cm² at 2.4 GHz (OET Bulletin 65)[3]. These caps stem from hard data: at 4 W/kg—50 times the FCC’s whole-body public limit—your core temperature climbs 1°C, stressing organs (IEEE C95.1)[4]. Push past 10 W/kg, and cataracts or skin damage loom (Elder, 2003)[5]. If RF why the regulations?
Now consider urban life, where RF is even more prevalent. A 30-minute phone call delivers 1 W/kg to your head, while towers cast 0.001–0.01 mW/cm² across streets. WiFi drenches you with 0.01–0.05 mW/cm² in homes and offices, blending into a daily 0.03 W/kg whole-body dose, with phone spikes hitting 1 W/kg locally (author’s estimate)[6]. That’s 63% of the FCC’s localized cap and 38% of its whole-body limit—technically “safe,” but perilously close. OSHA demands training and restricted zones for workers near these levels (29 CFR 1910.268)[8], a tacit nod that even “safe” isn’t benign. These standards are an admission of risk, but are silent on what issues decades of this exposure might breed. This may not be a surprise when you consider that there are billions in telecom profits hanging in the balance.
The ROS Cascade: A Cancer Trigger RF Could Ignite
The government regulations fixate (probably intentionally) on heat, assuming RF’s only sin is thermal. But cancer doesn’t need a flame—it grows from cellular chaos, and RF might spark that through a cascade of something called reactive oxygen species (ROS). These molecular troublemakers—hydroxyl radicals, superoxide, hydrogen peroxide—arise naturally in metabolism, but, in abundance, can become too much for the body to handle and eventually damage DNA, setting the stage for tumors. RF can’t ionize water like gamma rays, with their 10⁵ eV photons (IARC, 2011)[9] but it doesn’t need to. Studies suggest RF at urban levels—0.1–1 W/kg—can nudge ROS production without so much power.
Research like Yakymenko’s (2015)[10] shows RF at 0.1–1 W/kg—think phone calls or WiFi—boosting ROS in cells after hours. The mechanism isn’t heat but stress: oscillating fields might disrupt mitochondria, leaking superoxide from electron transport chains, or tweak enzymes like NADPH oxidase to churn out radicals. Over a day, 0.03 W/kg seems trivial—2,592 J/kg—but stretch that across 70 years, and it’s 180,000 J/kg, a relentless drip that could overwhelm antioxidants like glutathione (author’s calculation)[7]. Desai (2009)[11] found RF slashing sperm motility via oxidative stress at similar doses, hinting at broader cellular vulnerability. This isn’t ionization—it’s a slow grind, piling up ROS until DNA frays, mutations slip through, and cancer takes hold.
#### **Beyond ROS: Other Pathways to Cancer**
ROS isn’t the only issue with RF. Non-thermal effects could also pave cancer’s path. RF’s electric fields, even at 0.01–1 V/m in cities, might alter cell membranes or signaling, disrupting repair or growth controls. Panagopoulos (2011)[12] argues RF at 0.1 W/kg perturbs ion channels, skewing calcium fluxes that could misfire proliferation signals thus creating fertile ground for tumors. The National Toxicology Program (NTP) in 2018 found “clear evidence” of heart schwannomas in rats at 6 W/kg, with “equivocal” brain tumor hints at lower doses, suggesting RF might nudge cells toward malignancy without heat (NTP, 2018)[13]. The Ramazzini Institute (2018)[14] saw tumors at 0.1 W/kg—near urban reality—raising the specter of a threshold we’re flirting with daily.
Epidemiology adds weight to this argument. An Interphone study (2010)[15] linked heavy phone use—1 W/kg over 1,600 hours—to a 40% higher glioma risk (OR 1.4), while Hardell’s work ties brain tumors to long-term exposure (Hardell, 2013)[16]. Critics argue that these studies might suffer from recall bias but they certainly provide another credible signal demonstrating the need for further study (a signal being willfully ignored). RF might not break DNA directly, but by stressing repair systems or amplifying ROS, it could let natural errors compound into cancer over time.
The Profit Motive: A Veil Over Truth
So why isn’t this front-page news and why won’t our government study these potential health risks? Follow the money. Telecom hauls in over $1 trillion globally, with 5G alone projected at $700 billion by 2030 (Statista, 2023)[17]. The FCC’s limits, unchanged since 1996, lean on a thermal model telecom loves because the standards are easy to meet and hard to challenge… they provide cover. OSHA’s worker rules nod at risk but there’s no political will to learn information that could disrupt such a major industry. This can be demonstrated by the fact that when the NTP found tumors, telecom lobbies pounced, downplaying rat data as “irrelevant” (Wyde, 2018)[18]. Hardell’s warnings were buried under “more research needed” nonsense, a stall tactic straight from Big Tobacco’s playbook.
Urban exposure—0.03 W/kg daily over 70 years of life—hasn’t been tested long-term. The FCC’s 50-fold buffer below 4 W/kg is a guess, not a shield, forged when RF was a fraction of today’s flood (OET Bulletin 65)[3]. Give that cancer’s latency—20–50 years in asbestos or smoking (SEER, 2020)[19]—this means we’re in the danger zone now, 30 years post-cell phone boom. While I personally believe the foundational reason for the turbo cancers is the mRNA jabs, it is worth asking whether long-term exposure to high levels of RF radiation is also a contributing factor… but instead, telecom lobbying dollars continue to ensure that we remain guinea pigs while regulators shrug, citing “no proof”—a dodge based on their unwillingness to fund the research.
Conclusion: Cancer’s Quiet Seed
RF exposure may cause cancer—not immediately but with consistent exposure over a long period of time. An ROS cascade, sparked by chronic 0.03–1 W/kg doses, could erode DNA repair over decades, while non-thermal effects might miswire cells into malignancy. OSHA and the FCC admit RF’s risk with every limit, yet cling to heat as the sole foe, ignoring signals—NTP tumors, Hardell’s odds, Yakymenko’s ROS—these all scream for scrutiny. Sadly, telecom’s billions grease this silence, betting our health against their bottom line. We’re not frying, but we’re simmering, and cancer doesn’t need heat to bloom—just time and exposure. We need to demand the studies—our lives shouldn’t be their gamble.
Endnotes
1. Occupational Safety and Health Administration, “Non-Ionizing Radiation,” 29 CFR 1910.97. Available at: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.97. This regulation establishes a 10 mW/cm² limit for RF exposure in general industry settings.
2. Federal Communications Commission, “Radiofrequency Radiation Exposure Limits,” 47 CFR 1.1310. Available at: https://www.ecfr.gov/current/title-47/chapter-I/subchapter-A/part-1/subpart-I/section-1.1310. This sets public exposure limits, including 1.6 W/kg SAR and 0.08 W/kg whole-body.
3. FCC Office of Engineering and Technology, *Evaluating Compliance with FCC Guidelines for Human Exposure to Radiofrequency Electromagnetic Fields*, OET Bulletin 65, 1997. Available at: https://www.fcc.gov/oet/ea/documents/bulletins. Provides technical guidance on RF exposure limits and measurement.
4. IEEE Standard C95.1-2019, “Safety Levels with Respect to Human Exposure to Electric, Magnetic, and Electromagnetic Fields, 0 Hz to 300 GHz.” Published by the Institute of Electrical and Electronics Engineers. Details thermal thresholds, including the 4 W/kg mark for a 1°C temperature rise.
5. Elder, J.A., “Ocular Effects of Radiofrequency Energy,” *Bioelectromagnetics*, Supplement 6, 2003, pp. S148–S161. DOI: 10.1002/bem.10117. Documents high-dose RF effects like cataracts above 10 W/kg.
6. Author’s estimate based on typical urban RF measurements, consistent with examples in FCC OET Bulletin 65 and industry reports, reflecting levels from phones, towers, and WiFi. We ran this through Grok and other AI to come up with the number.
7. Author’s calculation derived from phone SAR (1 W/kg for 30 minutes daily) and ambient RF power density (0.01–0.05 mW/cm²), averaged over 24 hours, aligning with FCC guidelines. We also ran this through Grok and other AI to come up with the number.
8. Occupational Safety and Health Administration, “Telecommunications,” 29 CFR 1910.268(c). Available at: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.268. Requires training for workers exposed to RF hazards.
9. IARC, “Non-Ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields,” *IARC Monographs on the Evaluation of Carcinogenic Risks to Humans*, Volume 102, 2011. Available at: https://monographs.iarc.fr/wp-content/uploads/2018/06/mono102.pdf. Classifies RF as “possibly carcinogenic” (Group 2B).
10. Yakymenko, I., et al., “Oxidative Mechanisms of Biological Activity of Low-Intensity Radiofrequency Radiation,” *Electromagnetic Biology and Medicine*, Volume 34, Issue 3, 2015, pp. 186–202. DOI: 10.3109/15368378.2015.1043557. Reports ROS increases at 0.1–1 W/kg RF exposure.
11. Desai, N.R., et al., “Effects of Radiofrequency Electromagnetic Waves (RF-EMW) from Cellular Phones on Human Ejaculated Semen: An In Vitro Pilot Study,” *Fertility and Sterility*, Volume 92, Issue 4, 2009, pp. 1318–1325. DOI: 10.1016/j.fertnstert.2008.08.022. Links RF to oxidative stress in sperm.
12. Panagopoulos, D.J., et al., “Bioeffects of Mobile Telephony Radiation in Relation to Its Intensity or Distance from the Antenna,” *International Journal of Radiation Biology*, Volume 87, Issue 5, 2011, pp. 489–498. DOI: 10.3109/09553002.2011.560992. Proposes non-thermal RF effects on ion channels.
13. National Toxicology Program, “Cell Phone Radiofrequency Radiation Studies,” Technical Report, 2018. Available at: https://ntp.niehs.nih.gov/go/cellphone. Finds tumors in rats at 6 W/kg, with hints at lower doses.
14. Falcioni, L., et al., “Report of Final Results Regarding Brain and Heart Tumors in Sprague-Dawley Rats Exposed from Prenatal Life Until Natural Death to Mobile Phone Radiofrequency Field,” *Environmental Research*, Volume 165, 2018, pp. 496–503. DOI: 10.1016/j.envres.2018.01.037. Reports tumors at 0.1 W/kg.
15. INTERPHONE Study Group, “Brain Tumour Risk in Relation to Mobile Telephone Use: Results of the INTERPHONE International Case-Control Study,” *International Journal of Epidemiology*, Volume 39, Issue 3, 2010, pp. 675–694. DOI: 10.1093/ije/dyq079. Links heavy phone use to glioma risk.
16. Hardell, L., et al., “Mobile Phone Use and the Risk for Malignant Brain Tumors: A Case-Control Study on Deceased Cases and Controls,” *Pathophysiology*, Volume 20, Issue 2, 2013, pp. 85–92. DOI: 10.1016/j.pathophys.2013.03.001. Ties long-term RF exposure to brain tumors.
17. Statista, “Global Telecommunications Market Revenue Forecast 2023-2030,” 2023. Available at: https://www.statista.com/statistics/. Estimates telecom revenue, including 5G projections.
18. Wyde, M., et al., “Response to Criticism of the NTP Cell Phone Radiofrequency Radiation Studies,” *Environmental Health Perspectives*, Volume 126, Issue 8, 2018. DOI: 10.1289/EHP4168. Addresses industry pushback on NTP findings.
19. SEER Cancer Statistics Review, 1975–2020, National Cancer Institute, 2020. Available at: https://seer.cancer.gov/csr/1975_2020/. Provides cancer latency context.
*Tom Renz is a lawyer and commentator fighting for clarity in policy and law. Catch more at X @RenzTom. Also please consider supporting us by subscribing here and donating monthly at www.GiveSendGo.com/RenzLaw. And as always – check us out at www.TomRenz.com.
Covid mRNA “Vaccine” Cancer Risk: A Japanese Study Showing An Association Between Excess Cancer Mortality And The mRNA “Vaccine” Rollout Keeps Getting Censored 2ND SMARTEST GUY IN THE WORLD
MAR 16, 2025 – Just prior to the criminal FDA’s fraudulent approval of their Emergency Use Authorization (EUA) for the PSYOP-19 slow kill bioweapon “vaccines,” this Substack was sounding the alarm about the escalation of the global eugenics depopulation program.
The Modified mRNA platform could not pass a single animal study due to how dangerous it was, and yet somehow these poisons were foisted on the world at the height of what can only be termed the scamdemic.
“The greatest fear among vaccinologists is the creation of a vaccine that is not only ineffective, but which exacerbates disease. Unfortunately, CoV vaccines have a history of enhancing disease…” 2ND SMARTEST GUY IN THE WORLD
JANUARY 23, 2024
This article was originally published by this Substack on December 6th, 2021, and is now revised.
This Substack has been diligently chronicling the resulting VAIDS symptoms which every single genetically modified walking spike protein factory is, by varying degrees, afflicted with, and associated excess mortality surge.
From Turbo Cancer to Sudden Cardiac Mortality to Excess Non-Covid Natural Cause Mortality: The Never-Ending Adverse Events of the “Vaccinated” & The Global Depopulation Program 2ND SMARTEST GUY IN THE WORLD
JULY 9, 2023
Yesterday this Substack reviewed the latest cardiac mortality data:
Also covered was the horror show findings that the Modified mRNA “vaccine” was deliberately loaded with the highly carcinogenic SV40 promotor sequences.
CATASTROPHIC BOMBSHELL: First Ever Definitive Proof That Pfizer’s COVID “Vaccine” Integrates Into The Human Genome 2ND SMARTEST GUY IN THE WORLD
DECEMBER 6, 2024
And now we have additional proof that the SV40 was intentionally added to the “vaccines” as a kind of ticking time bomb bioweapon payload by both Pfizer and Moderna on behalf of their Intelligence Industrial Complex handlers, thus proving yet again that this whole PSYOP-19 program was an exercise in global bioterrorism:
Pancreatic Cancer Vitamin C & Ivermectin JUSTUS R. HOPE
Designing the Ultimate Repurposed Drug Protocol
MAR 16, 2025
When I began this journey five years ago, I was unaware of the top two Repurposed Drugs against Pancreatic Cancer, the disease that claimed my father’s life.
These two lifesaving drugs were never mentioned by his Oncologist, yet they were both used by Dr. Steven Bigelsen in 2015 against his Stage 4 Pancreatic Cancer, and they contributed to his complete remission. He remains alive and well today, and he continues to practice medicine some ten years later. I will discuss more on these two key drugs below.
But let us first begin with the #3 ranked drug. Dr. Paul Marik and I are closing in on a Pancreatic Cancer Repurposed Drug Protocol that AI says will provide a Moderate Likelihood of Inducing a Complete Remission from Stage 4 Pancreatic Cancer.
Let that sink in.
We are talking about a complete remission, not an improvement in survival of only a few months. Dr. Marik and I believe a substantial improvement is possible by adding this protocol to the standard of care.
And AI believes it is more than possible; AI believes it to be probable.
This protocol, if AI is correct, and I believe it is, will be a game changer in this disease.
The #3 Repurposed Drug against Pancreatic Cancer – MCP
Here is AI’s analysis on our tentative protocol – as revised – from changing Belapectin to Modified Citrus Pectin.
As we reviewed in our most recent Substack, Galectin-3 is highly expressed in Pancreatic Cancer, thus we theorized that a Galectin-3 blocker, whether Belapectin or MCP [Modified Citrus Pectin], should have a strong anti-metastatic effect. And you cannot find anything safer than an over-the-counter product derived from Orange Peels that blocks Galectin-3. So, adding MCP as part of the protocol was a no-brainer.
Why did I ask for AI to substitute MCP for Belapectin?
#1. Belapectin is not yet FDA approved for clinical use. It is unavailable.
#2. Assuming Belapectin is FDA approved, it will command “premium prices.”
AI reports that as a biologic, Belapectin would likely be priced in the thousands of dollars per year:
The most clinically tested MCP product is PectaSol, and it is priced at around 68 dollars for 120 tablets.
[Full Disclosure: I have no financial interest in this product]
In addition to MCP which AI ranks as the #3 most effective repurposed drug in the Pancreatic Cancer protocol, what are the six other drugs, and where do they rank and why?
The #4 Repurposed Drug against Pancreatic Cancer -Doxycycline
Beyond its antibiotic properties, doxycycline has demonstrated significant anticancer effects in pancreatic cancer models.
- In PANC-1 pancreatic cancer cells, doxycycline at concentrations of 20 μg/ml and above induced cell cycle arrest in the G1-S phase and triggered apoptosis through DNA fragmentation.
- The mechanism involves activation of p53 and p21 tumor suppressor genes and suppression of anti-apoptotic genes like Bcl-xL and Mcl-1.
- In a mouse xenograft model, doxycycline treatment suppressed pancreatic tumor growth by 80%, suggesting strong in vivo efficacy.
- It also demonstrated the ability to suppress both endogenous and chemotherapy-induced IL-8 expression, which could help combat therapy resistance.
AI ranks it #4 in our protocol.
But on to our favorite repurposed drug which AI ranks at #5 against Pancreatic Cancer.
The #5 Repurposed Drug against Pancreatic Cancer – Ivermectin
March 16, 2025 Pressured by mandates? Don’t give in. Opt out.
Enjoy the latest single from Green Family Productions. Quality entertainment for people who dare to think.
A remarkable cancer treatment has been hiding in plain sight for decades A Midwestern Doctor
Story at a Glance:
- Dimethyl sulfoxide (DMSO) effectively treats a broad spectrum of conditions, including strokes, pain, tissue injuries, autoimmune inflammation, and cancer.
- DMSO inhibits cancer growth and consistently reverts cancer cells to their normal state.
- DMSO enhances cancer visibility to immune cells, enabling the body to eliminate tumors previously undetected by the immune system.
- DMSO effectively mitigates major challenges in conventional cancer care, such as radiation damage, chemotherapy toxicity, and pain from “incurable” metastatic cancer.
- DMSO markedly boosts the efficacy of many chemotherapy drugs, allowing safer, lower doses to achieve the same results.
- When paired with certain natural therapies, DMSO often produces highly effective cancer treatments, revolutionizing cancer care. [Emphasis added]
Cancer is one of the most challenging conditions to deal with in medicine, as two seemingly identical cancers can have very different causes. As a result, any standardized (holistic or conventional) protocol will inevitably fail some of the patients it is meant to treat.
Furthermore, since there is so much fear surrounding cancer (e.g., from what the primal fear brings up inside you, from how your social circle reacts to it and from how the medical system uses all of that to push cancer therapies) it is often very difficult to have a clear head about the ordeal or find the right source of advice.
Likewise, since so much money is involved (e.g. 65% of oncologist’s revenues comes from chemotherapy drugs and cancer drugs are by far the most profitable drug market), there is significant pushback (e.g. from medical boards or unhappy relatives) against anyone who attempts alternative cancer therapies making it very difficult to practice unconventional cancer care—particularly since no alternative treatment works all the time.
Note: in a recent article, I highlighted how urologists initially would not touch Lupron (which is now also used as a the puberty blocker) because of how unsafe and ineffective it was, but once they started being paid a lot of money to prescribe it for prostate cancer, it rapidly became their number one drug.
In contrast, while the conventional cancer therapies often have serious issues that make them far worse than any benefit they offer, some conventional cancer therapies are frequently the only available option which can save someone’s life (which has led to me at different times having fights with close friends or relatives either not to do chemotherapy or to get them to start it in cases where I felt it was absolutely necessary).
Given all of this, I presently believe that no “ideal” cancer treatment exists, but if it can be done (e.g., it’s effective for the cancer and feasible to implement), the most ideal to least ideal treatments are as follows:
•Identifying the root cause of a cancer, removing it, and having it quickly and permanently go away on its own (which is sometimes possible).
•Have enough time to rebalance the body so that its terrain no longer supports the cancer and the cancer can fade away on its own (which is often doable but a fairly involved process many have difficulty carrying out).
•Significantly enhance the function of the immune system so that it will eliminate the cancer.
•Find a treatment that is toxic to the cancer but relatively benign to the rest of the body.
•Find a treatment with an acceptable toxicity level and find ways to mitigate its effects.
•Accept a moderately toxic treatment with significant side effects.
•Focus on living with the cancer rather than curing it and then finding ways to mitigate the symptoms you experience both from it and any existing treatment protocols.
•Use a costly conventional therapy that is unlikely to work and live with all the side effects until your life ends (which in more extreme treatment regimens can be quite severe).
If we take a step back, what’s truly remarkable about DMSO, depending on how it is used, is that it can effectively provide most of the benefits listed above with the least amount of collateral damage (e.g., side-effects, toxicity, etc.).
Dimethyl Sulfoxide (DMSO)
Exactly six months ago, I used this newsletter to bring the public’s attention to DMSO, a simple naturally occurring compound that has a number of immense therapeutic benefits and virtually no toxicity (detailed here). In turn, when it was discovered in the 1960s, it quickly became America’s most desired drug (as it cured many incurable ailments). A lot of the scientific community promptly got behind it and before long, thousands of papers had been published on every conceivable medical application for it. Consider for example this 1980 program 60 Minutes aired on DMSO:
Dr. Peter McCullough is getting a lot wrong about bird flu, and it is important that his bad advice be corrected. Meryl Nass, M.D.
Sorry, Peter, but could your Wellness Company’s product sales be influencing your fear-mongering?
March 14, 2025 – Dr. Peter McCullough has an interview out today with John Solomon on Real America’s Voice. Both the channel and Dr. McCullough are financially tied to The Wellness Company. Dr. McCullough is its Chief Scientific Officer.
The Wellness Company sells kits to prevent bird flu (avian influenza) including potentially useful nasal and throat sprays, and sells oseltamvir (Tamiflu). Tamiflu is a prescription antiviral medication that barely works for ordinary influenza. It can reduce symptoms by only 16 hours if you take it at the first sign of flu. It does not stop or prevent the infection. Taken later, it does nothing, though it can cause many side effects, including suicidal thoughts and suicide. Not a drug to be taken lightly.
It was used on the teenage girl who became seriously ill from bird flu in Canada, but did not help.
Dr. McCullough is selling Wellness Company kits for farmers to prevent bird flu. I have no problem with the nasal and throat sprays, but I have a big problem with including tamiflu in the kits, because people will take it at will, and some will have serious side effects. And so far, there is no evidence it does anything for bird flu in humans.
According to the CDC, 70 Americans have had bird flu in the US—ever. That number has not changed in 3 or 4 weeks. One got really sick and died, but it is not clear if it was due to bird flu. The Louisiana health department was agnostic about the cause of death, stating it was related to bird flu but not due to bird flu:
Here are the total human cases identified in the US: (chart)
Dr. McCullough said bird flu is taking a turn for the worse. He is entirely wrong about this. Why?
- He says the virus “has now spread” to 40 different types of mammals. Actually, I reported on the many types of mammals that could be affected by bird flu months ago, using old USDA data, with a map showing which animals had been found with bird flu throughout the US. Since bird flu is spread by migrating birds, and is very contagious, it can be found in many animals. Certain animals, like seals and cats, can get very ill, while most migrating birds and many other animals are usually asymptomatic.
- In the last 3 weeks, only 200,000 poultry total have been culled in the US, according to CDC, averaging about 10,000/day. During the last 2 months of the Biden administration, nearly a million birds were being culled daily, 100 times more.
- He advises not to drink raw milk. However, both USDA and CDC say that bird flu is not a food-borne illness. There have been NO cases of bird flu ever reported due to drinking infected milk or eating dairy products (or anything else), even though we know that some affected raw milk made it into the food chain. There are antiviral substances in raw milk. If you wish to drink it, go ahead. The only way FDA and USDA were able to find live, viable bird flu virus in raw milk was after they put it there themselves in an experiment.
- No new human cases have surfaced in about a month
- All recovered, apart from the Louisiana case. Nearly all had only pink eye or mild respiratory symptoms.
- CDC directed hospitals to test their severe flu cases for bird flu, and 6 cases turned up. But no details were ever provided. It is unclear if these were false positive tests.
- While both the Canadian teenager and the Louisiana person who died were the only critically ill people identified in North America with bird flu, both had the D1.1 genetic type (genotype). It is often found in wild birds, and now several dairy herds have been found with this type of bird flu. However, it turns out that about 14 dairy workers also had this type of D1.1 bird flu, but they only had mild symptoms. Most of the rest of the affected herds and people had the B3.13 genotype. Whether we need to worry more about D1.1 is not clear yet, but given the rarity of human cases recently, things are looking good.
- Since there have been no new severe cases identified in the past two months, and just a handful of mild cases identified this year, Dr. McCullough is wrong to scare people that human to human spread is just around the corner. There has never been a proven case of human to human spread of bird flu. There are several possible cases, but they occurred years ago. Even possible cases never spread to more than one or two people, at most. There is no reason to think bird flu, which has probably been around forever, will suddenly acquire the ability to spread between humans. That is, unless it gains that ability in a laboratory.
So please relax, avoid oseltamvir (tamiflu) and don’t worry about bird flu. I am monitoring it closely, and if the situation changes, I will immediately let people know.
Medical CEO, Three Others Arrested After 5-Year-Old Boy Is Incinerated in Hyperbaric Chamber Inferno By Jack Davis
March 15, 2025 The Western Journal – Three people have been charged with second-degree murder in connection with the January death of a 5-year-old boy in a hyperbaric chamber that burst into flames at a Michigan clinic.
Thomas Cooper died on Jan. 31 at the Oxford Center, in Troy. His mother, who was with him at the time, suffered burns after the chamber caught fire, killing the child.
Oxford Center CEO Tami Peterson, safety director Jeff Mosteller and primary manager Gary Marken were all charged with second-degree murder, according to WXYZ-TV.
Aleta Moffitt, who operated the hyperbaric chamber, was charged with one count of involuntary manslaughter and intentionally providing false information on a medical record.
“This tragedy could have been prevented if proper safety protocols were followed,” Michigan Attorney General Dana Nessel said.
“Instead, deliberate negligence and a blatant disregard for safety cost a child his life. I appreciate the investigatory efforts of the Troy Police Department. My office remains committed to seeking justice for Thomas and holding those responsible accountable.”
In a statement, the Oxford Center said it was “disappointed to see charges filed.”
“The timing of these charges is surprising, as the typical protocol after a fire-related accident has not yet been completed. There are still outstanding questions about how this occurred. Yet, the Attorney General’s office proceeded to pursue charges without those answers,” the statement said.
James Harrington, the attorney for the family, said the boy had received multiple hyperbaric treatments for sleep apnea and attention deficit disorder, according to NBC.
Harrington said the family will file a lawsuit in addition to the criminal charges.
“This is a very, very egregious case,” Harrington said.
“A single spark it appears ignited into a fully involved fire that claimed Thomas’s life within seconds,” Nessel said, according to the Associated Press.
“Because these treatments were so medically unsound, patient insurance policies would not cover the use of these chambers to treat these conditions,” Nessel said. “This business was a pure cash-flow, for-profit business.”
Hyperbaric treatment gives an individual five times the level of oxygen normally present, and if approved by the Food and Drug Administration for treating severe burns and wounds and decompression sickness.
The FDA list of approved treatments does not include conditions for which the Oxford Center used hyperbaric therapy.
Nessel said on the day of the boy’s death, no maintenance check was performed, no medical doctor was present, and treatment was not being led by a licensed technician.
The 5G Safety Myth: Assumed Safe, Not Proven Safe NICOLAS HULSCHER, MPH
Despite insufficient safety data and growing evidence of biological effects, 5G and other wireless technologies are being deployed unchecked, prioritizing corporate interests over public health.
MAR 15, 2025
NICOLAS HULSCHER study titled, The assumption of safety is being used to justify the rollout of 5G technologies, published in Frontiers in Public Health, reviews the existing safety literature of fifth-generation (5G) wireless communication technology:

The Assumption of Safety in 5G Deployment
- The study argues that the rollout of 5G is based on an assumption of safety rather than conclusive scientific evidence.
- Government and industry stakeholders have misinterpreted scientific uncertainty as an indication that no risks exist.
- The lack of long-term health data on 5G mmWave exposure is being used to justify widespread deployment rather than as a reason for caution.
Biological and Health Risks of 5G mmWave Exposure
The study highlights findings from existing literature suggesting biological effects, including:
- Oxidative Stress – Increased production of reactive oxygen species, which can lead to inflammation and cellular damage.
- Immune System Effects – Potential impacts on immune function, raising concerns about biological responses to long-term exposure.
- Genotoxicity – Evidence of DNA damage in some studies, though findings are not universally consistent.
- Neurological Effects – Some research suggests possible changes in neuronal activity, warranting further investigation.
- Cellular Disruption – Increased cell membrane permeability, which may influence various biological processes.
FDA Admits Covid mRNA ‘Vaccines’ Cause Cancer Frank Bergman
February 13, 2025 – The U.S. Food and Drug Administration (FDA) has just made the explosive admission that Covid mRNA “vaccines” are spiked with contaminations that triggered a global surge in cancers.
The federal agency made the admission after an FDA study confirmed that Pfizer’s Covid mRNA “vaccine” contains dangerous levels of excess DNA contamination.
As Slay News previously reported, leading scientists have been warning for some time that surges in deadly cancers among the Covid-vaccinated were caused by DNA fragments in the mRNA injections.
Those warnings have now been confirmed in a bombshell study conducted in the FDA’s own laboratory.
Tests conducted at the FDA’s White Oak Campus in Maryland found shocking levels of DNA contamination in the “vaccines.”
The residual DNA levels exceeded regulatory safety limits by 6 to 470 times.
While six times the safe limit would be alarming, 470 times is unprecedented and devastating.
The vaccine vials used during the study were sourced from BEI Resources.
BEI is a trusted supplier affiliated with the National Institute of Allergy and Infectious Diseases (NIAID), previously headed by Dr. Anthony Fauci.
The findings of the peer-reviewed study were published in the Journal of High School Science.
The study finally shuts down years of dismissals by regulatory authorities, who had previously labeled concerns about excessive DNA contamination as baseless.
The FDA is expected to comment on the findings this month.
However, the agency has yet to issue a public alert, recall the affected batches, or explain how vials exceeding safety standards were allowed to reach the market.
The FDA researchers employed two primary analytical methods:
- NanoDrop Analysis – This technique uses UV spectrometry to measure the combined levels of DNA and RNA in the vaccine. While it provides an initial assessment, it tends to overestimate DNA concentrations due to interference from RNA, even when RNA-removal kits are utilized.
- Qubit Analysis – For more precise measurements, the researchers relied on the Qubit system, which quantifies double-stranded DNA using fluorometric dye.
Both methods confirmed the presence of DNA contamination far above permissible thresholds.
These findings align with earlier reports from independent laboratories in the United States, Canada, Australia, Germany, and France.
Kevin McKernan, a former director of the Human Genome Project, described the findings as a “bombshell.”
In a statement, he blasted the FDA for its lack of transparency.
“These findings are significant not just for what they reveal but for what they suggest has been concealed from public scrutiny,” McKernan said.
“Why has the FDA kept these data under wraps?”
In addition to genome integration, McKernan highlighted another potential cancer-causing mechanism of DNA contamination in the vaccines.
He explained that plasmid DNA fragments entering the cell’s cytoplasm with the help of lipid nanoparticles could overstimulate the cGAS-STING pathway.
The cGAS-STING pathway is a crucial component of the innate immune response.
“Chronic activation of the cGAS-STING pathway could paradoxically fuel cancer growth,” McKernan warned.
“Repeated exposure to foreign DNA through COVID-19 boosters may amplify this risk over time, creating conditions conducive to cancer development.”
Adding to the controversy, traces of the SV40 promoter were detected among the DNA fragments.
While the authors concluded that these fragments were “non-replication-competent” meaning they cannot replicate in humans, McKernan disagreed.
“To assert that the DNA fragments are non-functional, they would need to transfect mammalian cells and perform sequencing, which wasn’t done here,” McKernan stated.
“Moreover, the methods used in this study don’t effectively capture the full length of DNA fragments,” he added.
“A more rigorous sequencing analysis could reveal SV40 fragments several thousand base pairs long, which would likely be functional.”
McKernan has been one of the leading voices sounding the alarm over the cancer-causing DNA in the Covid “vaccines.”
As Slay News previously reported, McKernan issued a warning to the public last month after discovering traces of Covid mRNA “vaccines” in the rapidly developing cancerous tumors of turbo cancer patients.
Dr. McKernan, a genomics scientist with 25 years of experience in his field, made the discovery during experiments in his Boston lab.
Continue reading
Study of 99 Million Confirms Covid ‘Vaccines’ Caused Global Death Surge Frank Bergman
March 15, 2025 Slay News – A major peer-reviewed study of almost 100 million people has confirmed that Covid mRNA “vaccines” have caused a global surge in death and deadly disease.
The study documents the outcomes of 99 million people after they received Covid mRNA injections.
During the study, the researchers examined the official government data from eight countries.
Participants in the study included 99,068,901 Covid-vaccinated individuals.
The study has concluded that the injections are responsible for the global surge in sudden deaths and life-threatening illnesses.
The researchers found that staggering numbers of vaccinated people suffered serious complications such as heart failure, blood clots, strokes, brain disorders, and severely weakened immune systems.
Many of those tracked by the peer-reviewed study also died suddenly and unexpectedly.
The research was conducted by the Global Vaccine Data Network in New Zealand.
The study’s paper was published in the prestigious, world-renowned Vaccine journal.
Over the past three years, the study has documented the outcomes for 99 million people who were given Covid shots.
As Slay News has previously reported, multiple studies from around the world have now linked the injections to various complications.
The most common serious medical side effects have been blood clots and myocarditis, both of which can be fatal.
Myocarditis is the inflammation of the heart muscle (myocardium), according to the Mayo Clinic.
The inflammation reduces the heart’s ability to pump blood.
The condition weakens the heart so that the rest of the body doesn’t get enough blood.
Clots can form in the heart, leading to a stroke or sudden cardiac arrest.
Now, after studying almost 100 million vaccinated people, the new study has confirmed that “the shots from pharma giants, including Pfizer, Moderna, and AstraZeneca have been associated with rare occurrences of heart, brain, and blood disorders.”
Participants from eight different countries were monitored for upticks in 13 medical conditions.
The study revealed that besides a slight increase in neurological issues, the vaccines were also associated with dangerous blood and heart-related medical conditions.
The researchers discovered soaring numbers of people suffering from myocarditis after doses of Pfizer-BioNTech’s and Moderna’s mRNA shots.
However, medical experts have repeatedly warned that those suffering from myocarditis are rarely aware that they have it until it’s too late, creating a ticking time bomb situation among the members of the public.
The study showed those getting AstraZeneca’s viral-vector shot had a 6.9-fold increased chance of pericarditis, an inflammation of the cardiac muscle.
The lead author of the study’s paper is Kristýna Faksová of the Department of Epidemiology Research at the Statens Serum Institute in Copenhagen, Denmark.
Speaking about the results of the study, Faksová said:
“The size of the population in this study increased the possibility of identifying rare potential vaccine safety signals.
“Single sites or regions are unlikely to have a large enough population to detect very rare signals.”
Faksová’s study uncovered evidence of “an elevated risk” of developing a specific blood clot type in the brain.
This increased risk was linked to Covid shots like the one produced by the University of Oxford and distributed by AstraZeneca.
Further, recipients of AstraZeneca’s contribution to the shot pool were 2.5 times more likely to get Guillain-Barre syndrome.
Guillain-Barre syndrome is a neurological disorder in which the body’s immune system attacks nerves.
According to the study, the development of Guillain-Barre syndrome also creates a risk of transverse myelitis, an inflammation of the spinal cord, and other complications with the brain and spinal column.
Evidence of myocarditis, which is inflammation of the heart muscle, was particularly recurrent among individuals after their first, second, or booster dose of an mRNA vaccine.
Modest spikes in incidence were noted, especially following the administration of the second dose of the Moderna shot, which was also tied to a raised occurrence of pericarditis after initial and booster vaccinations.
The researchers also warn of the incidence of cerebral venous sinus thrombosis, a once-exceptionally rare type of cerebral clot.
This has already prompted many countries to discontinue using AstraZeneca‘s shots.
Meanwhile, a group of leading scientists in Germany has raised the alarm after discovering evidence buried in the German government’s official data that confirms excess deaths were caused by mRNA “vaccines” and not Covid.
The bombshell study provides yet further confirmation that excess mortality rates did not rise during the first waves of the pandemic, despite official claims of surging “Covid deaths.”
Excess mortality rates did skyrocket, however, but only after the Covid mRNA “vaccines” were rolled out for the public.
Interestingly, the study found that the most significant excess mortality event during the pandemic period was not caused by Covid at all but by a late 2022 influenza wave.
Excess deaths spiked due to people dying from the flu after they received Covid mRNA “vaccines.”
READ MORE – FDA Admits Covid mRNA ‘Vaccines’ Cause Cancer
Comments
Comments are closed.